
Feldene

Allen Ray Sing Chen, M.D., M.H.S., Ph.D.
- Associate Professor of Oncology

https://www.hopkinsmedicine.org/profiles/results/directory/profile/0008071/allen-chen
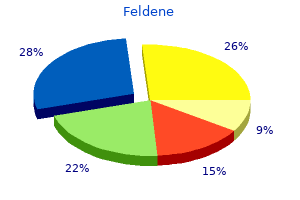
A small tube is inserted through the eardrum to keep the hole open for a longer time diffuse arthritis definition discount feldene 20mg amex. These tubes usually remain in place for 6 to 18 months and may fall out by themselves prevent arthritis in hands fingers cheap feldene 20mg without a prescription. If he/she has pain anti-arthritis diet for dogs buy feldene with visa, you may give the recommended dosage of acetaminophen (Tylenol) arthritis pain vinegar order feldene 20 mg with visa. There may be some blood tinged drainage on the cotton placed in the ear after surgery arthritis in the knee and swelling discount feldene express. Diet/Activity Immediately after surgery rheumatoid arthritis quiz order generic feldene, your child will do best with a liquid diet. On the day after surgery, your child may return to usual activity, including school and daycare. Begin using these drops on the evening following surgery, as directed by your doctor. Place drops of into: Right ear Left ear Both ears times each day for days. If the drainage continues for more than seven days, or if other symptoms arise such as fever or pain, please call our office at (415) 353-2148. When using the drops, warm them first by holding the bottle in the hand for a few minutes. After placing the drops, pump the front of the ear next to the opening of the ear canal several times. Keep the bottle after you have finished the prescribed amount since you may be able to re-use this medication if your child develops an ear infection (drainage from the ear) in the future. Ear infections the primary purpose of tubes is to provide additional ventilation to the ear and thereby decrease the frequency of ear infections. Drainage from the ear, which may be thin, thick, or blood-tinged, is the most common sign of infection. Your primary care physician can successfully treat these infections with ear drops. If drainage persists despite ear drops, oral antibiotics may need to be prescribed. You will also need to call the Pediatric Otolaryngology clinic at (415) 353-2757 to schedule a follow-up appointment with a hearing test. If there are any problems or questions that arise before that time, please call the office at (415) 353-2148. Although they have reviewed the report, neither they nor their organizations necessarily endorse its fndings or conclusions. We would further like to thank those who participated on the expert panel that developed the antibiotic reduction targets that serve as the foundation for this report: Eva Enns, Thomas File, Jonathan Finkelstein, Jefrey Gerber, Adam Hersh, Jefrey Linder, Ruth Lynfeld, David Margolis, Larissa May, Daniel Merenstein, Joshua Metlay, Jason Newland, Jay Piccirillo, Daniel Shapiro, Katie Suda, Ann Thomas, and Teri Moser Woo. Additionally, the project team would like to thank the following Pew colleagues for their assistance in the development of this report. Thanks to Tia Carter, a former colleague, for help in coordinating and convening the expert panel; and to Sarah Despres for lending her expertise to this efort. Finally, thanks to Heather Cable, Katie Portnoy, Laurie Boeder, Demetra Aposporos, Bailey Gregory, and Dan Benderly for providing valuable feedback and production assistance on this report. Pew applies a rigorous, analytical approach to improve public policy, inform the public, and invigorate civic life. Contents 1 Overview 2 Background Importance of improved antibiotic stewardship 2 3 Establishing a baseline of outpatient antibiotic use 5 Establishing national targets for reducing unnecessary antibiotic use in outpatient settings Overarching recommendations for reduction 8 Acute respiratory conditions 8 Sinus infections 9 Middle ear infections 10 Pharyngitis 11 Viral upper respiratory infections 12 Bronchitis and bronchiolitis 13 Asthma and allergy 13 Infuenza 14 Pneumonia 15 Other conditions 16 17 Reaching national targets for improved antibiotic use: the role of antibiotic stewardship Outpatient antibiotic stewardship: What does it look like These drugs should be used only to treat bacterial infections and, when needed, the right antibiotic should be prescribed at the most appropriate dose and duration. Yet antibiotics are often prescribed inappropriately across health care settings in the United States. Antibiotic stewardship eforts, which aim to ensure that these drugs are prescribed appropriately, are critical for combating the public health threat posed by antibiotic-resistant pathogens. To efectively implement and evaluate stewardship eforts, it is essential to frst understand current antibiotic prescribing patterns. Antibiotic use in outpatient health care settings, such as primary care ofces and emergency rooms, represents the majority of dollars spent on antibiotics for human health care in the United States. Approximately 13 percent of all outpatient ofce visits in the United States, or about 154 million visits annually, result in an antibiotic prescription; about 30 percent of these, or some 47 million prescriptions, are unnecessary. Half of these prescriptions are unnecessary, since many are viral illnesses or other conditions that do not respond to antibiotics. This report is the frst in a series evaluating current antibiotic use in the United States and establishing national targets for improved prescribing practices in diferent health care settings. In addition to these fndings, the expert panel discussed the importance of increased stewardship activities to ensure that the United States reaches the goal laid out in the 2015 national action plan. There is no one-size-fts all stewardship program that practitioners can implement in their facilities. However, a number of interventions have been shown to be efective at improving prescribing habits, such as providing clinicians with individualized antibiotic prescribing feedback. Since no single agency or organization oversees antibiotic use in outpatient facilities across the country, implementing stewardship programs nationwide will be a complex undertaking. A diverse group of stakeholders will need to take coordinated and sustained action to provide the resources and expertise necessary to expand stewardship eforts. However, the emergence and spread of antibiotic-resistant bacteria threaten the efectiveness of these critical therapies. According to the World Health Organization, high rates of resistance in common bacteria are being seen worldwide. To minimize this threat and preserve the efectiveness of these important drugs, antibiotics should be used judiciously and prescribed only when recommended. In addition to the importance of antibiotic stewardship in minimizing the threat of resistance, reducing inappropriate antibiotic use can also improve patient safety. It is estimated that antibiotic-related adverse events result in more than 140, 000 emergency room visits a year. These diagnoses collectively accounted for 44 percent of all outpatient antibiotics, representing 68 million prescriptions per year. Many of these respiratory syndromes are caused by viruses or may resolve without an antibiotic. Acute respiratory conditions are clearly in need of additional stewardship activities. Figure 1 Outpatient Antibiotic Prescriptions by Diagnosis Acute respiratory conditions % % Sinus infections 44 25 Acute % Middle ear respiratory 22 infections conditions % Pharyngitis 20 % Viral upper 12 respiratory infections % Bronchitis/ 12 bronchiolitis % Pneumonia % 5 (nonviral) 56 % Asthma/allergy Other conditions 4 Note: Not pictured are infuenza and viral pneumonia. There are not enough visits with an antibiotic prescribed in the data set to calculate reliable estimates for these diagnoses individually. Both diagnoses do contribute to the total number of antibiotics prescribed for acute respiratory conditions. Children younger than 2 receive the most antibiotics, averaging just over one prescription per child per year. Although these variations do not necessarily indicate inappropriate antibiotic prescribing, they highlight populations for which targeted stewardship eforts may have the greatest efect. Participants were chosen based on their expertise in appropriate outpatient antibiotic use and represented a wide range of specialties, such as primary care, infectious diseases, pediatrics, emergency medicine, pharmacy, nursing, and public health. Using the baseline antibiotic-use data presented above, the experts reviewed the prescribing rates and current practice guidelines for each diagnosis to determine how much antibiotic use could be eliminated for each (see Appendix C for additional information on methodology for setting reduction targets and Appendix D for recommended reduction targets). This condition-specifc approach allowed the panel to factor in variations in antibiotic prescribing guidelines between each illness when setting reduction targets. Margolis University of Pennsylvania Dermatology Larissa May University of California, Davis Emergency medicine Daniel Merenstein Georgetown University Family medicine Joshua Metlay Massachusetts General Hospital Internal medicine, epidemiology St. Louis School of Medicine Otolaryngology Rebecca Roberts Centers for Disease Control and Prevention Public health Guillermo Sanchez Centers for Disease Control and Prevention Public health, physician assistant Daniel Shapiro University of California, San Francisco Biostatistics Katie Suda University of Illinois at Chicago Pharmacy, infectious diseases Ann Thomas Oregon Health Authority Public health, pediatrics Teri Moser Woo Pacifc Lutheran University Pediatric nursing, nurse practitioner prescribing Rachel Zetts the Pew Charitable Trusts Public health, epidemiology 5 Figure 4 Expert Panel Recommendations for Improving Outpatient Antibiotic Use Proportion of unnecessary antibiotic use: All conditions Unnecessary vs. Appropriate Use, by Health Condition Miscellaneous bacterial Nonviral pneumonia Urinary tract infections Middle ear infections infections* (suppurative) % % % % 100 100 100 13 % 30 % 87 Unnecessary use Remaining conditions** Sinus infections Pharyngitis Asthma/allergy % % % 18 100 70 % Appropriate 34 % % use 51 49 % % 82 66 Bronchitis/bronchiolitis Middle ear infections In uenza Viral pneumonia (nonsuppurative) % % % % 100 100 100 100 National goal for reducing inappropriate antibiotic use by 2020 50 percent reduction, or approximately 23 million fewer prescriptions, by 2020 Viral upper respiratory infections Nearly 47 million % 100 unnecessary antibiotic prescriptions each year 0 10 20 30 40 50 60 70 80 90 100 6 Proportion of unnecessary antibiotic use: All conditions Unnecessary vs. The majority of this reduction would come from eliminating unnecessary antibiotic prescribing for acute respiratory conditions. The panel determined that half of all antibiotics prescribed for these conditions are unnecessary, leading to about 34 million excess prescriptions annually. Acute respiratory conditions should clearly be a target of antibiotic stewardship eforts in outpatient settings. Additionally, improving prescribing practices for other conditions, such as skin infections and acne, could reduce antibiotic use by about 13 million prescriptions annually. Figure 5 Outpatient Antibiotic Prescribing Reduction Targets 100 % 15 80 Reduction 86. Sinus infections Sinus infections are the most common reason that antibiotics are prescribed in outpatient settings in the United States, accounting for more than 17 million prescriptions annually. Although sinus infections can be caused by a number of pathogens, both bacterial and viral, treatment guidelines recommend antibiotic use only when the infection is suspected to be caused by bacteria. The panel recommended a geographic approach to setting reduction targets for prescribing antibiotics to treat sinus infections. Using this method, the ideal antibiotic prescribing rate for sinus infections was set to match the U. The panel estimated that nearly 6 million unnecessary antibiotic prescriptions are written for sinus infections each year. Adult patients account for an overwhelming majority of these and should be the primary population targeted by stewardship eforts for this diagnosis. It will be important to evaluate progress made toward these targets and to assess whether further reduction goals are warranted. About 15 million antibiotic prescriptions are written for this diagnosis each year, with 87 percent of them for patients 19 and younger. As with sinus infections, antibiotics are only sometimes recommended for treating this diagnosis. The symptoms associated with middle ear infection may be caused by a true infection (suppurative otitis media, identifed by the presence of pus) or by the presence of noninfected fuid in the middle ear (nonsuppurative otitis media). Based on current practice guidelines, the panel recommended eliminating all antibiotic prescribing for nonsuppurative cases of middle ear infections. For a suppurative diagnosis, the panel used the same approach as with sinus infections, setting the target prescribing rate to match that of the lowest prescribing region. Based on this method, the panel estimated that there are nearly 2 million unnecessary prescriptions written for suppurative middle ear infections each year. Antibiotic stewardship activities should focus on improving prescribing for middle ear infections in children and adolescents, as this population accounts for such a large proportion of antibiotics prescribed for this diagnosis. Additionally, stewardship eforts should focus on helping providers to accurately diagnose suppurative middle ear infections, because these are the only cases for which antibiotics may be needed and overdiagnosis of suppurative cases may contribute to overprescribing. This condition accounts for over 13 million outpatient antibiotic prescriptions a year in the United States. Ensuring appropriate diagnostic testing for strep throat is critical to improving antibiotic use for this diagnosis. These infections are caused primarily by viral pathogens, and current guidelines recommend against prescribing antibiotics. This population is a key target for antibiotic stewardship eforts for acute bronchitis. As with infuenza, an individual estimate of this reduction in millions of antibiotic prescriptions could not be calculated because of data limitations. For nonviral pneumonia, the panel did not recommend any reduction target because antibiotic therapy is recommended for this diagnosis. Others, such as acne and skin infections, only sometimes warrant antibiotic treatment. For these conditions, the panel again recommended using a regional approach to set reduction targets.
The laparoscopic surgeon inspects for some injury signs like abdominal pain arthritis back mayo cheap feldene online mastercard, unexplained fever arthritis in neck of horse cheap feldene 20mg mastercard, abdominal distension and altered bowel function chinese arthritis relief hand movements generic 20mg feldene amex. Treatment consists of a transversally bowel resection of all necrotic area with end-to-end anastomosis arthritis pain in elbow buy feldene 20 mg visa, lavage and antibiotics arthritis pain and relief discount 20 mg feldene fast delivery. Rupture of superficial or deep vessels to the anterior abdominal wall can Robotic Surgery Versus Abdominal and Laparoscopic Radical Hysterectomy in Cervical Cancer 39 cause bleeding and hematoma arthritis in fingers nodules purchase 20 mg feldene otc. Therefore, this damage should be avoided by placement of the trocar with the laparoscopic visualization to the rectus muscles. Treatment depends on the location of the injury as well as the damage is arterial or venous. The greatest amount of clinical experience has been with use of a through-and-through loop of suture around the bleeding site (Harris, 1997; Jhingran & Levenback, 2007; Kim, 2007; Li, 2007; Reich, 2011; Rhodes, 1999; Tang & Obermair, 2009). Thus, the laparoscopic surgeon and the vascular surgeon must perform direct laparatomy and repair the blood vessels. If any instruments are faulty within the abdomen, it should be withdrawn from the abdomen laparoscopically in the majority of cases. The indication for the role of laparoscopy in the future will be determined by the increased familiarity of gynecologic surgeons with these procedures. There is no major difference between robotic-assisted hysterectomy and the laparoscopic hysterectomy regarding postoperative considerations and complications (Basil & Pavelka, 2011). Robotic surgery provides all the benefits of the laparoscopic technique with greater precision and effectiveness. However, we have to point out several considerations about the equipment and about how the robotic system works. The da Vinci System allows gynecologists to performed hysterectomies more precise than conventional surgery. Robotic surgery is useful for the treatment of gynecologic cancers and other conditions such as fibroids, vaginal prolapsed (Beste, 2005; Reich, 2011; Stovall & Mann, 2011). The technique may also be applied for several other therapeutic indications such as sacral colpopexy, tubal reanastomosis, endometriosis and pelvic pain (Cadiere, 2001; Basil & Pavelka, 2011; Reich, 2011; Stovall & Mann, 2011). Moreover, the variety of procedure is easier because of 3-dimensional visualization (Cadiere, 2001; Reich, 2011). The da Vinci and Vinci S Robotic Systems are currently used (Cadiere, 2001; Chitwood; 2001; Reich, 2011; Stovall & Mann, 2011). Four main trocars are currently used including a 12 mm transumbilical trocar, two trocars of 8 mm placed at 10 cm to the right and left of the umbilical one, while the last trocar is positioned 10 cm lateral and 5 cm caudal to the right robotic trocar, respectively. The assistant trocar of 10 mm is located 3 cm cranial to the umbilical and left trocar. After removal of the specimen, a colpo-occluder balloon is placed in the vagina to maintain pneumoperitoneum (Chitwood; 2001; Reich, 2011; Scott, 1999; Stovall & Mann, 2011). The robotic system is a technique that uses a remote control, two interactive mechanical arms and a 3D-image processing system, being considered the greatest advance in surgery in the past decades. The motions of the surgeon are translated to the robotic arms by using the remote control unit, whereas the robotic arms hold interchangeable surgical instruments that can be moved in a specific manner. Although the robotic system has progressed from simple surgical tasks to more complicated surgery in the past decade, robotic surgery is still in stage of development (Cadiere, 2001; Degueldre, 2000; Diaz-Arrastia, 2002; Stovall & Mann, 2011). The da Vinci Robotic Surgical System uses 7 degrees of freedom of motion by the combination of the instruments wrists and the abdominal wall trocar positioned arms. Robotically assisted gynecologic procedures are generally performed using a combination of remote control, foot pedals and hand controls. These include hand control for operating the instruments, one pedal which is capable to move camera resulting in precise orientation and focus on and a second pedal for repositioning and centering the hand controls. The surgeons first performed bilateral tubal ligations with robotic assistance before progressing to total hysterectomies using the system. The da Vinci System offers some improvements over traditional laparoscopy: 3-dimensional images, hand tremors and dexterity limitations, but the additional costs, set-up time and limited tactile feedback are major boundaries. In some cases, adequate hemostasis is not advisable with ultrasonic energy; bipolar cautery should be used to assure hemostasis before dividing the entire cardinal ligament (Breda, 2001; Rhodes, 1999; Reich, 2011; Scott, 1999; Stovall & Mann, 2011). Robotic Surgery Versus Abdominal and Laparoscopic Radical Hysterectomy in Cervical Cancer 41 the gynecologic surgeon should master the anatomy of female reproductive tract and the intricacy of lower urinary tract, large intestins and internal genital organs to avoid key surgical complication. Abdominal hysterectomy Abdominal hysterectomy is a surgical procedure in which the surgeon detaches the uterus from the ovaries, fallopian tubes and upper vagina, as well as from the blood vessels and connective tissue (Baggish & Schellhas, 2011; Beste, 2005; Carlson, 1994; Jhingran & Levenback, 2007; Scott, 1999). The uterus is a hollow thick walled, muscular organ located in the lower abdomen and pelvis of the female. The lower portion of the uterus namely the cervix may be removed (total hysterectomy), but also may be left in place (partial or supracervical hysterectomy) (Baggish & Schellhas, 2011; Beste, 2005; Carlson, 1994; Jhingran & Levenback, 2007; Scott, 1999). At its upper end, the uterus narrows into the fallopian tubes and end by curling around the ovary. The decision concerning appropriate therapy and extent of the abdominal hysterectomy should be made by the woman in consultation with the surgeon for a number of conditions (Baggish. All women with any uterine bleeding before or after menopause should undergo evaluation (Jhingran & Levenback, 2007; Reich, 2011; Scott, 1999). Fibroids produce symptoms of prolonged and excessive regular uterine bleeding; besides, fibroids may cause pelvic pain and excessive bleeding or pressure (Jhingran & Levenback, 2007; Reich, 2011; Scott, 1999). Pelvic muscles and ligaments are often weakened by vaginal childbirth and other pelvic trauma, life-style factors, chronic constipation and aging process. The patient should not undergo hysterectomy until all ulcers of cervix and vagina are healed. If 42 Hysterectomy necessary, vaginal or abdominal hysterectomy is performed carefully with a vaginal vault suspension (Jhingran & Levenback, 2007; Reich, 2011; Scott, 1999). An abdominal or vaginal hysterectomy is rarely needed (Jhingran & Levenback, 2007; Reich, 2011; Scott, 1999). Simple or complex hyperplasia without atypia can often be treated with medication. For older patients with complex atypical hyperplasia and those who fail progestin therapy, the risk of developing endometrial cancer is increased. Classic or laparoscopic surgery is the primary treatment modality for carcinoma of uterus, cervix or ovaries. In addition, radiation therapy alone may be used in patients with significant medical comorbidities. In addition, the surgeon should combine laparoscopic hysterectomy with laparoscopic lymphadenectomy. In patients with stage I grade 1 tumors an extrafascial total abdominal hysterectomy with bilateral salpingo-oophorectomy is always recommended. Furthermore, postoperative irradiation can be used if myometrial invasion to the outer third is diagnosed. In patients with stage I grades 2 and 3 tumors the use of paraaortic lymphadenectomy has gained popularity over the last years. Postoperative radiation is recommended for grade 2 or 3 tumors that invade the myometrium, full pelvic irradiation offering some benefit (Carlson, 1995; Jhingran & Levenback, 2007; Scott, 1999). Therapeutic options may vary depending on the histologic type of endometrial carcinoma. Cytotoxic therapy may provide a potential benefit, while radiotherapy may be useful for patients who underwent operation as primary therapy. However, the patient should have a routine preoperative evaluation (Carlson, 1995; Jhingran & Levenback, 2007; Scott, 1999). Traditional radical hysterectomy includes removal of the uterus and cervix, one third of the vagina, the parametrial tissue at the pelvic sidewall and ligature of utero-sacrals (Carlson, 1995; Jhingran & Levenback, 2007; Reich, 2011; Scott, 1999; Stovall & Mann, 2011). Recently, there has been a great interest in laparoscopic surgery regarding treatment in carcinoma of the cervix. These procedures permit a through exploration of the abdomen and the tumor itself. In considering the therapy of cervical carcinoma, patient suspected of having cervical carcinoma should first have biopsy of the tumor. The diagnosis of microinvasive cervical cancer cannot be established by biopsy of the tumor, therefore a cervical conisation must be performed. Occasionally, conisation can be used as safe therapy if the margins are free of tumor. These are equally effective as treatments for minimal spread to the vagina (Carlson, 1995; Jhingran & Levenback, 2007; Reich, 2011; Scott, 1999; Stovall & Mann, 2011). In fact, some investigators have reported that the carcinoma of the cervix is closely associated with endometrial cancer. It should be noted that patients with cervical carcinoma characteristically present symptoms such as bleeding, back pain, loss of appetite, weight loss and a history of not having had a cervical cytology (pap smear) for a long period. However, women with late menopause, a history of nulliparity and late 44 Hysterectomy childbearing appear to have an increase in risk for ovarian cancer (Carlson, 1995; Reich, 2011; Scott, 1999; Stovall & Mann, 2011). In case of benign epithelial ovarian tumors like serous cystadenoma, hysterectomy and bilateral salpingo-oophorectomy are usually performed. As well, mucinous tumors can lead to the deposits in the peritoneal cavity by perforation and rupture. Adenofibromas are also treated by simple excision, while Brenner tumors are rare and almost benign, therefore oophorectomy is usually proposed. When these tumors occur in perimenopausal or postmenopausal period, hysterectomy and bilateral salpingooophorectomy offers the best treatment option. Most of the ovarian tumors can be approached surgically through a Phannenstiel incision or by laparoscopic excision. After the diagnosis of malignancy is established by histologic examination of tumor tissue excised at operation, a second procedure can be performed (Jhingran & Levenback, 2007; Scott, 1999; Stovall & Mann, 2011). The most common borderline ovarian tumors tend to occur in young women aged between 38 and 45 years old (Markovska & Grabowski, 2009). Fertility sparing surgery with abdominal cavity inspection and biopsy of peritoneum and controlateral ovary is indicated (Markovska & Grabowski, 2009). Mucinous borderline tumors are frequently associated with large amounts of mucinous material in the peritoneum; sometimes, an appendiceal adenoma or an appendiceal carcinoma which require appendectomy is identified. Based on these findings, surgery offers the best treatment for such tumors (Jhingran & Levenback, 2007; Scott, 1999; Stovall & Mann, 2011). Biopsy and cytologic evaluation is performed to obtained samples from the peritoneum or any suspicious nodules. Current evidence suggests that paraaortic and pelvic lymphnodes sampling is indicated (Benedetti, 2008; Benedetti, 2009). Additionally, surgical treatment may involve splenectomy, diaphragmatic stripping, posterior exenteration and bowel resection (Harris, 1997; Jhingran & Levenback, 2007; Scott, 1999; Stovall & Mann, 2011). Robotic Surgery Versus Abdominal and Laparoscopic Radical Hysterectomy in Cervical Cancer 45 4. In addition, the pelvic and paraaortic nodes biopsies is currently performed (Jhingran & Levenback, 2007; Scott, 1999; Stovall & Mann, 2011). Postoperatively, three options are currently available in such cases: no postoperative treatment, postoperative radiation and postoperative chemotherapy. Moreover, certain studies have concluded that such therapy is able to improve the performance status. However, several other prospective and retrospective studies have suggested that many patients with negative second look operation develop recurrent disease. On the other hand, it is important for women with chronic pelvic pain to ask about the probability that her pain will improve after hysterectomy. Also, laparoscopic presacral neurectomy should be reserved for the patients with significant pain refractory to an adequate trial of conservative treatment. In addition, heart rate, blood pressure loss and respiration are closely observed before general or spinal anesthesia is given (Jhingran & Levenback, 2007; Reich, 2011; Scott, 1999). There are several types of 46 Hysterectomy hysterectomy procedures and it is possible for a less invasive procedure to be performed, such as a laparoscopic hysterectomy or a vaginal hysterectomy. These procedures are not practical for complications; in such cases, therefore, the surgeon will made than likely have to revert to an abdominal hysterectomy. Simple abdominal hysterectomy differs from radical hysterectomy with pelvic lymphadenectomy. The ureter should be identified and dissected after the peritoneum is entered by clamped, cut and sutured-ligated the round ligament. At this point, the peritoneum, the tissue containing lymphnodes and fat are all dissected and the psoas muscle, external iliac vessels and the ureter identified. The external iliac artery, external iliac vein and internal iliac artery are cleared of fat. Second, the obturatory artery and nerve are cleaned of fat and lymphnodes (Baggish & Schellhas, 2011; Meeks and Harris, 1997; Reich, 2011; Rhodes, 1999; Scott, 1999; Stovall & Mann, 2011). When the node dissection of the external iliac and of the obturator fossa is complete, the operator turns to the common iliac node dissection. Next, the uterine arteries are clamped, cut and suture-ligated distal to their origin from the hypogastric arteries. Also, at the place where the ureter penetrates the cardinal ligaments to the wall of the bladder, a right angle clamp should be inserted between the ureter and cardinal ligament. When the ureter is clearly free and mobile, the bladder pillars are clamped, cut and sutured. At that point, the vesico uterine and retrouterine spaces should be dissected down-ward bellow the cervix and the utero-sacral ligaments are clamped, cut and suture-ligated (Baggish & Schellhas, 2011; Meeks and Harris, 1997; Reich, 2011; Rhodes, 1999; Scott, 1999; Stovall & Mann, 2011).
Generic 20mg feldene with visa. Dr Joel Wallach explains Rheumatoid Arthritis.
Cao Ma-Huang (Ephedra). Feldene.
- Improving athletic performance, allergies, asthma and other breathing disorders, nasal congestion, colds, flu, fever, and other conditions.
- Is Ephedra effective?
- Weight loss. Ephedra can produce modest weight loss when used with exercise and a low fat diet, but it can cause serious side effects, even in healthy people who follow product dosage directions.
- How does Ephedra work?
- Dosing considerations for Ephedra.
- Are there safety concerns?
- What is Ephedra?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96822
It is the nature of any document whether published in a traditional format or on-line that it can very quickly become out of date arthritis medication cream purchase discount feldene on-line. At the time of publication (December 2015) arthritis pain relief australia feldene 20mg generic, all hyperlinks have been checked and are complete arthritis pain keeps me awake at night discount feldene 20 mg without prescription. We would also like to again take this opportunity thank all the contributors and editors of previous editions of the Guidelines who have provided us with such a firm foundation on which to build arthritis fingers blister purchase feldene visa. Sonographers are qualified healthcare professionals who undertake arthritis diet to prevent feldene 20 mg online, report and take responsibility for the conduct of diagnostic can arthritis in neck cause back pain purchase feldene american express, screening and interventional ultrasound examinations. Sonographers also perform advanced diagnostic and therapeutic ultrasound procedures such as biopsies and joint injections. They are either not medically qualified or hold medical qualifications but are not statutorily registered with the General Medical Council. Individuals without a recognised qualification, including student sonographers should always be supervised by qualified staff. A sonographer should: i) recognise and work within their personal scope of practice, seeking advice as necessary; ii) ensure that a locally agreed and written scheme of work is in place; iii) work with reference to national and local practice and guideline recommendations; iv) ensure they hold appropriate professional indemnity insurance or obtain this by virtue of their employment (ref: section 1. The registration situation for sonographers is complex 1 the majority of sonographers are statutorily registered but this will depend on their professional background and is not achievable for all. Government policy since 2011 has been not to bring further aspirant groups into statutory registration unless there is a clear evidence of clinical risk that requires this. Autonomy and accountability for healthcare workers, social care workers and social care workers. The majority of statutorily registered ultrasound practitioners will already meet this requirement and will not need to take any further action. They will either work in an employed environment where their employer will indemnify them, and / or if they undertake self-employed work, they will have already made their own professional indemnity arrangements. However, some statutorily registered ultrasound practitioners may need to take steps to make sure that they have appropriate professional indemnity arrangements in place. Registrants and applicants for statutory registration will be asked to confirm that they meet, or will meet, this requirement by completing a professional declaration when renewing or registering for the first time. Ultrasound practitioners who are self employed or who work in a part employed, part self-employed environment are particularly advised to read the guidance published by their statutory regulator. There is no professional indemnity insurance associated with voluntary registration on the Public Voluntary Register of Sonographers. If an ultrasound practitioner is not statutorily registered, it is clearly good practice to ensure that they have appropriate professional indemnity arrangements in place both to protect the public and themselves. There is published advice on education and training available to those who use ultrasound in this way but whose main work and role is not that of an ultrasound practitioner. It is important for safe and effective service delivery that all ultrasound examinations are undertaken by appropriately trained and competent personnel and that there is associated audit and continuing professional development in the use of ultrasound. There is no evidence that diagnostic ultrasound has produced any harm to patients in the four decades that it has been in use. However, the acoustic output of modern equipment is generally much greater than that of the early equipment and, in view of the continuing progress in equipment design and applications, outputs may be expected to continue to be subject to change. Also, investigations into the possibility of subtle or transient effects are still at an early stage. Doppler imaging and measurement techniques may require higher exposures than those used in B and M-modes, with pulsed Doppler techniques having the potential for the highest levels. Recommendations related to ultrasound safety assume that the equipment being used is designed to international or national safety requirements and that it is operated by competent and trained personnel. It is the responsibility of the operator or ultrasound practitioner to be aware of, and apply, the current safety standards and regulations and to undertake a risk/benefit assessment for each examination. Key principles for the safe use of ultrasound: 2 i) Medical ultrasound imaging should only be used for medical diagnosis. Their content should address the ultrasound examinations, their reporting and the appropriate referral pathways for patients with normal and abnormal ultrasound findings. The details in the protocols should be such that a new staff member, having read them, could carry out and report these examinations and appropriately refer the patient after the examination to the expected standard. Protocols should be updated regularly and their review date should be included in their content. Records are currently required by law to be kept for a number of years as specified by Department of Health advice (ref: section 2. Examples would be the image storage requirements of the abdominal aortic aneurysm and fetal anomaly screening programmes and those published by the Department of Health. It advises ministers in all four countries and is part of Public Health England, an executive agency of the Department of Health. Guidance on when ultrasound examinations of the neonatal hip should be performed can be found at. Public Heath England advice on private screening for different conditions and diseases. Information outlining the advantages and disadvantages of screening outside the national programmes can be found via the following web link. There is information and leaflets available for healthcare professionals and links to leaflets written for patients. There are several causative factors including high workloads, increasing body mass index of patients, poor equipment 13 and room design and poor posture when scanning. It is important that ultrasound practitioners take care of themselves and their working environment whilst scanning. Employers have a legal duty of care to their employees and should be guided in ways to avoid potential work related injuries i. Many advice and guidance documents have been published to which ultrasound practitioners are referred: Health and Safety Executive Risk management of musculoskeletal disorders in sonography work (2012). Manufacturers can set these up to your requirements at the time of installation and will optimise features such as transducer frequency and harmonics. Firm pressure may be contra-indicated for some types of pathology or clinical situations. In addition, some patients may have a clear preference for a health carer of specific gender due to their ethnic, religious or cultural background, because of previous experiences or in view of their age. Where possible such individual needs and preferences should be taken into consideration. When required, private, warm, comfortable and secure facilities for dressing and undressing should be provided. Care should be taken to ensure privacy in waiting areas used by patients not fully dressed in their own clothes. During the ultrasound examination, only those body parts under examination should be exposed. Care must be taken to maintain confidentiality when non-health care personnel are nearby. The ultrasound practitioner should give equal consideration to their own need for a chaperone, again irrespective of the examination being undertaken or the gender of the patient. A record should be made in patient records when chaperones are offered and used, and when they are declined. There are several organisations that have produced advice on the conduct of intimate examinations and also on the use and role of chaperones. Society and College of Radiographers (2011) Intimate Examinations and Chaperone Policy. Time needs to be allowed for room preparation, assessing the ultrasound request, introductions, explanations, obtaining consent and assisting the patient when necessary on to and off the examination couch. Post procedure time is required to discuss the findings with the patient, write the report, archive the images and attend to the after-care of the patient, including making arrangements for further appointments and/or further investigations. An ultrasound practitioner has a professional responsibility to ensure that the time allocated for an examination is sufficient to enable it to be carried out competently. It is critical to patient management that no ultrasound examination is compromised by departmental and or government targets. It may also be influenced by the expertise of the ultrasound practitioner and training commitments within the department. In addition, the duration of the examination will be further influenced by the scan findings and/or the physical condition of the patient. Examination times will need to take into account whether there are trainees present and their stage of training if teaching is to be effective. The time allocation for appointments to meet these requirements is a minimum of twenty (20) minutes. The time allocation for appointments to meet these requirements for a singleton pregnancy is a minimum of thirty (30) minutes and for a multiple pregnancy is forty five (45) minutes. The Society and College of Radiographers has published guidance on examination times at. Individual departments can determine examination times taking into account local circumstances. For example, it may be necessary to perform both transabdominal and transvaginal scans to fully evaluate the female abdomen and pelvis with ultrasound. Valid informed consent must be obtained before commencing any ultrasound examination or procedure. Ultrasound practitioners who do not respect the right of a patient to determine what happens to their own body in this way may be liable to legal or disciplinary action. The consent process is a continuum beginning with the referring health care professional who requests the ultrasound examination and ending with the ultrasound practitioner who carries it out. It is the responsibility of the referring professional to provide sufficient information to the patient to enable the latter to consent to the ultrasound examination being requested. It is the responsibility of the ultrasound practitioner to ensure that the patient understands the scope of the ultrasound examination prior to giving his or her consent. Additional informed verbal consent should be obtained where a student ultrasound practitioner undertakes part or all of the ultrasound examination under supervision. Verbal informed consent for those examinations of an intimate nature should be recorded in the Ultrasound report. Some categories of ultrasound examination (interventional ultrasound, guided procedures. The following are all relevant: Royal College of Radiologists Standards for patient consent particular to radiology (2012). By safeguarding high standards of care and seeking to continuously improve its quality, it ensures that health care provision is patient centred which is central to the concept. The main components of a clinical governance framework can be summarised as follows: 3 i) Risk management ii) Clinical audit iii) Education, training and Continuous Professional Development iv) Patient and carer experience and involvement v) Staffing and staff management An example of published Trust information on clinical governance can be found at. This will include audit of ultrasound examinations and reports: participation in multi-disciplinary team meetings and radiology discrepancy meetings would be further examples; ii) Communication and consent: (ref: section 1. This is of particular importance following the publication of the Francis Report in 2013 4 (ref: section 1. The National Ultrasound Steering Group was a short-term sub-group of the National Imaging Board. Web links Standards for the provision of an ultrasound service (2014). The on-line training sessions enhance traditional learning, support existing teaching methods and provide a valuable reference point. They are designed and built to be engaging and interactive, using quality images, video, audio 20 and animation to help trainees learn and retain knowledge.
The most relevant carcinogens produced by cooking Carcinoma of the bladder has been linked with the manufacture of dyes arthritis pain formula tylenol buy cheap feldene on line, rubber arthritis relief ankle purchase feldene 20mg, paint arthritis in neck and lower back cheap 20mg feldene free shipping, and aromatic amines arthritis in the back joints order feldene 20mg fast delivery. Higher is associated radioactive decay of uranium eitrige arthritis definition purchase cheap feldene, can be trapped in with gastrointestinal arthritis pain relief cvs purchase feldene with paypal, reproductive, renal, and homes, and is carcinogenic to humans. Chapter 10 Cancer Epidemiology this page intentionally left blank 11 Cancer in Children Foundational objeCtives have a peak incidence before the child is 5 years of age. Central nervous sys reproduction and differentiation and determine tem tumors are more common in children younger than their specific anatomical site selection. Bone tumors, soft tissue sarcomas, and lympho Review Foundational Objectives in Chapter 9. Describe the genetic etiologic factors After studying this chapter, the learner will be able to for childhood cancers. Describe the incidence and types of childhood Some environmental and host factors predispose a cancers. Childhood An analysis of cancer incidence rates for children 0 cancer most likely can be attributed to the complex inter to 19 years of age by primary site for all types of child action of both genetic and environmental factors. The statistics showed rates per 100, 000 individu tions, single-gene defects, or chromosome abnormali als. For children with this syndrome, the risk for devel kidney, and the lymphatic system. Thus, the more com opment of leukemia is 10 to 20 times greater during the mon childhood cancers are leukemias, sarcomas, and first 10 years of life than the risk is in healthy children. Embryonic tumors originate during Wilms tumor is particularly recognized for its intrauterine life and contain immature tissue unable to association with a number of genitourinary malfor mature or differentiate into functional cells. Embryonic mations, congenital absence of the iris of the eye, tumors are diagnosed early, usually by 5 years of age. Approximately 10% of children diagnosed with cancers usually result from environmental carcinogens Wilms tumor demonstrate one of these abnormalities. Retinoblastoma, a malignant embryonic increase between the ages 15 and 19 years and become tumor of the eye, occurs as an inherited defect or as the most common cancer type after adolescence. Single-gene defects have been associated mia, accounting for more than one third of childhood with the subsequent development of childhood tumors. The second most common group is cancers of Two autosomal recessive diseases involving increased the nervous system, primarily brain lesions. All other chromosomal fragility, Fanconi anemia and Bloom pediatric malignancies occur much less often. Rhabdomyosarcoma lance system during intrauterine life may explain the is a soft tissue sarcoma of striated muscle. During rapid prolifera bone tumors, osteosarcoma and Ewing sarcoma, occur tion and differentiation of cells in the developing fetus, in children. Childhood cancers usually are diagnosed during peak A few malignancies seem to demonstrate a familial times of growth and maturation. Chapter 11 Cancer in Children has a risk for leukemia that is two to four times greater chemotherapy, multimodal treatment for childhood solid than that for a child with a normal sibling. The occurrence tumors, improvement in supportive care, and develop of leukemia in monozygous twins is estimated as being ment of research centers for childhood treatment. These late effects are suppressor gene, the risk for development of cancer in more significant in children than in adults because child childhood or adulthood is significantly higher than that hood treatment occurs in a physically immature, growing in the unaffected population. The incidence for adult cancers is much higher than Study page 291; refer to Table 11-5. In childhood cancers, the ori ing radiation have been linked to subsequent cancers. The prognosis is of the vagina has developed in a small percentage of the better for children than adults. Childhood exposures to drugs, ionizing radiation, and viruses have been implicated as risk factors for PraCtiCe examination specific cancers. Drugs implicated include: (1) anabolic True/False: androgenic steroids, which are used in the treatment of aplastic anemia or used illegally by teenaged athletes 1. Childhood cancers are more common than adult for body development and have been associated with cancers. Childhood cancers have a strong relationship to may predispose a child to leukemia in later years; and environmental agents. Among childhood cancers in Caucasian children, cancer therapy and, possibly, their genetic constitution. Childhood cancers have more long-term able treatments and are better able to tolerate the imme consequences than adult cancers. Childhood cancers have a better prognosis than rates in pediatric oncology are the use of combination adult cancers. The overall incidences of cancer are nearly equal in Caucasian and Hispanic children. Fewer than 50% of children diagnosed with cancer can expect to survive for 5 years. Identify the structures responsible for maintaining and protecting the central nervous After reviewing this chapter, the learner will be able to system. Compare the functions of neurons with those of Review pages 310, 311, and 313; refer to Figures neuroglia; identify the parts of neurons. Describe the circumstances under which nervous Review pages 311-313; refer to Figure 12-24. Identify the three main divisions of the brain; Review pages 313 and 316; refer to Figures 12-25 characterize their associated structures and through 12-27. Identify the significance of contralateral control Review pages 317, 320, and 321; refer to Figures of motor fibers. Describe the location and structure of the spinal functional changes that occur with aging. The composition of cerebrospinal fluid is: body and a single axon at the other end of the cell a. Elicits rest-response Match the effect of sympathetic nerve stimulation with the structure: 23. Sensory nerves transmit the stimuli from pain receptors into the dorsal horn of the spinal cord. The impulses ascend by either the neospinothalamic tract or the paleospinothalamic tract. The paleospinothalamic tract carries information to the midbrain and is responsible for reflex responses to pain, thus changing autonomic func tion. The neospinothalamic tract carries information to the lateral thalamus and then projects to the cortex, where precision and discrimination occur. Afferent stimulation of the ventromedial medulla and periaqueductal gray mat ter in the midbrain stimulates efferent pathways, which modify or inhibit afferent signals to the dorsal horn. Cells in the substantia gelatinosa of the dorsal horn function as a gate and permit some impulses to reach the central nervous system for interpretation. In addition to gate control through stimulation of large and small fibers, the central nervous system, through its efferent pathways, may close, partially close, or open the gate. The sensory-discriminative system is mediated by the somatosensory cortex and identifies the presence, character, location, and intensity of the pain. The affective-motivational system determines conditioned avoidance behaviors and emotional response to pain. Pain modulation increases or decreases the transmission of pain throughout the nervous system. This gate control theory does not explain chronic pain problems such as phantom limb pain. The neuromatrix theory of pain proposes that in the absence of discernable causes for chronic pain, the brain pro duces nerve impulses triggered from the periphery or they originate independently within the brain. All endorphins attach to opiate receptors on the plasma membrane of the afferent neuron. The com bination of the opiate receptor and endorphin inhibits the release of excitatory neurotransmitters, thereby blocking the transmission of the painful stimulus. Thermoreceptors provide the hypothalamus with information about peripheral and core temperatures. If the temperature is low, the body initiates heat conservation measures by a series of hormonal mechanisms. Epinephrine causes vasoconstriction, glycolysis, and increased metabolic rates, which increase heat production. Decreasing the sympathetic pathway produces vasodilation, decreased muscle tone, and increased perspiration. Elderly individuals have poor responses to environmental temperature extremes as a result of slowed blood circula tion, changes in the skin, and an overall decrease in heat-producing activities. Many neurotransmitters are associated with excitatory and inhibitory sleep patterns. Awake-promoting neurotransmitters include hypocretin, acetylcholine, and glutamate. The sleep patterns of the newborn and young child vary from those of the adult in total sleep time, cycle length, and percentage of time spent in each sleep cycle. Sleep for infants and children is important for growth and neurocognitive development. It becomes transparent at the cornea in the central anterior region, which allows light to enter the eye. The choroid is the pigmented middle layer that prevents light from scattering inside the eye. The iris, part of the choroid, has a round opening, the pupil, through which light passes. Nerves from the nasal halves of the retinas cross and join fibers from the temporal halves of the retinas to form the optic tracts. The optic tracts connect to the primary visual cortex in the occipital lobe of the brain. Light entering the eye is focused on the retina by the lens, which is a flexible, biconvex, crystal-like structure. The aqueous humor of the anterior cavity helps maintain pressure inside the eye and provides nutrients to the lens and the cornea. The vitreous chamber is filled with a gel-like vitreous humor that prevents the eyeball from collapsing inward. The external structures protecting the eye include the eyelids, conjunctiva, and lacrimal apparatus. Sound waves entering the external auditory canal cause the tympanic membrane to vibrate. Three ossicles transmit the vibration of the tympanic membrane to the inner ear and set the fluids of the inner ear in motion. The bony labyrinth is divided into the cochlea, the vestibule, and the semicircular canals. Receptor cells on the basilar membrane are stimulated and transmit impulses along the cochlear nerve, a division of the vestibulocochlear nerve, to the auditory cortex of the temporal lobe for sound interpretation. In the semicircular canals, the dynamic equilibrium receptors respond to changes in direction of movement. Both of these impulses are transmitted through the vestibular nerve, a division of the vestibulocochlear nerve, to the cerebellum. After studying this chapter, the learner will be able to Neuropathic pain results from abnormal process do the following: ing of sensory information by the peripheral and central nervous systems. Describe clinical categories of pain; characterize lesion or dysfunction in the brain or spinal cord, such pain threshold and pain tolerance. Study pages 327-329; refer to Figure 13-4 and Tables Peripheral pain is the result of trauma or disease that 13-2 through 13-4. The pain threshold is the lowest intensity at which Psychogenic pain is pain without a known physical a stimulus is perceived as pain and may be influenced cause.
References
- El-Orbany M, Connolly LA. Rapid sequence induction and intubation: current controversy. Anesth Analg. 2010;110(5):1318-1325.
- Kennedy OD, Schaffler MB. The roles of osteocyte signaling in bone. J Am Acad Orthop Surg 2012; 20(10):670-1.
- Martis CS. Complications after mandibular sagittal split osteotomy. J Oral Maxillofac Surg 1984;42:101.
- Larsen SM, Levine LA: Review of non-surgical treatment options for Peyronieis disease, Int J Impot Res 24:1n10, 2012.
- McDonald OG, Owens GK: Programming smooth muscle plasticity with chromatin dynamics, Circ Res 100(10):1428-1441, 2007.