
Doxycycline
Beri M. Ridgeway, MD
- Staff, Center of Urogynecology and Reconstructive Surgery, Department of
- Obstetrics and Gynecology, Obstetrics, Gynecology, and Women? Health
- Institute, Cleveland Clinic, Cleveland, Ohio
Patient access schemes will be necessary to remain competitive in an increasingly saturated market even for drugs that are deemed to be innovative antimicrobial resistance in developing countries cheap 200mg doxycycline mastercard. There is an opportunity for manufacturers to offer discounts at the formulary level in order to get preferred formulary positioning antimicrobial growth promoters order doxycycline online from canada. Cosentyx has been approved for first line in Europe so we need to see how these compare to Cosentyx antibiotic 9 letters cheap 200 mg doxycycline. Datamonitor Healthcare surveyed five formularies that were chosen based on a combination of factors antibiotic 294 purchase doxycycline uk, including largest impact and patient population size antibiotic resistance conjugation cheap generic doxycycline canada, to understand the formulary decisions behind key psoriasis drugs antibiotic vaginal itching 200 mg doxycycline with amex. Dovobet more effective than models comparing topical treatment analogs (tacalcitol, should not be used single therapy various treatments calcitriol), longer than four alone and is cost to Dovobet as first topical weeks effective with line therapy with corticosteroids, comparators. Bristol, North Somerset, and South Gloucestershire Health Community (2015) Bristol, North Somerset and South Gloucestershire Health Community local formulary. Price assumptions Datamonitor Healthcare uses national formularies to gather pricing information per product. As the prices presented in formularies can differ, showing prices at different stages in the supply chain, Datamonitor Healthcare uses backing-out formulas to adjust formulary prices in order to obtain estimates of ex-factory wholesale prices. These prices are the retail price exclusive of consumption tax, therefore it is important to note that the sales given for Japan may be inflated compared to other countries, depending on the extent of price markups at different stages in the supply chain. However, Datamonitor Healthcare has validated its patient-based sales estimates with company-reported sales in Japan where available, and believes the impact to be minimal. Patented Medicine Prices Review Board (2012) 2011 Backing-Out Formulas for Foreign Price Verification. This document is a licensed product and is not to be reproduced or redistributed. All patients in this series complained of typical skin manifestations of psoriasis. Simultaneously the clinical manifestations of psoriasis improved and finally disappeared. It was slightly reduced at the end of third month was later maintained near the initial level (109. The improvement therefore of the clinical status of the patients was most likely because of restoration of serum zinc level to normal. Key Words: Zinc deficiency, copper deficiency, erythrocyte zinc content, atomic absorption spec trophotometry. Despite this long history of the ailment and the fact part in etiopathogenesis of psoriasis (9-16) and further that nearly 3% of population in United States suffers from more contribute significantly to its treatment. Common cal examination was performed on each patient upon arrival factor between the patient with psoriasis and animals with (Table 1). If the clinical impression supported the former diagno parakeratosis is, however, reduced serum zinc levels (7). No case was given observation led us to start a program of trace metal treat our specified treatment until the diagnosis was histologically con ment on these patients the preliminary results of which firmed. Several ointments all containing samples for trace element measurements were removed and cortisone derivatives were prescribed by physicians without processed with appropriate precautions to prevent contamina much success. Her complaints started eight years ago on the lateral No changes occurred in the lesions during the first month of aspect of the I. They used to alleviate during summer months second month, and the lesions appeared hyperemic. Scaling 50% reduction in the size of the lesions during the third month lesions then appeared behind the ears and forehead. Only few 3x4 mm lesions remained at the end of abnormalities were encountered in physical examination. Sedimentation rate patients is the fact that in no case classical or newly proposed was 37 mm/h. A biopsy was performed report of which revealed antipsoriasis medicaments were prescribed. Tur molar region, and during the third month 10x15 mm lesion at the pentine, anthimony, cantharides and phosphorus were I. She first complained of itching and scaling lesions at was considered standard treatment (4). X-rays were later both pre-tibial skin 3 years ago following; which typical scaling proposed to treat psoriasis. This method was soon dis psoriatic lesions appeared gradually extending to the prepateller carded however, because of its well known side effects. Before Treatm ent During Treatm ent M ean values of subsequent visits First m onth Second m onth Third m onth Cases Serum 1010 E Serum Serum 1010 E Serum Serum 1010 E Serum Serum 1010 E Serum Serum 1010 E Serum Zn E Zn Zn Cu Zn E Zn Zn Cu Zn E Zn Zn Cu Zn E Zn Zn Cu Zn E Zn Zn Cu D. This was further But because of carcinogenic effects of ultraviolet rays and confirmed when it was noted that the patients suffering ocular and immunological complications this method has from psoriasis became somewhat better during the recently fallen into disfavor (20, 21). But its side effects during the long effects, were actually not very influential in treatment of periods of treatment has widely precluded its application psoriasis (2). One of the latest developments in treatment of psoria Peckham and his associates conducted a wide scale sis involves trace elements. Review of literature from this study inquiring about the then current therapy of psoriasis point reveals many communications assigning a signifi in 1976. Of the 510 dermatologists contributing, 52% cant role to trace metals in pathogenesis of psoriasis (9 stated that methotrexate was the most frequently utilized 16). In fact several authors in the past have reported low chemotherapeutic agent (18). During the last 10 years the serum zinc levels in patients with psoriasis, while others most favorable treatment has been methotrexate with or have found it within normal limits. After clinical and laboratory studies a biopsy of one were below normal values (Table 1). The serum zinc restore them to normal, copper supplementation was levels were determined (Table 2) following which the resorted to (32, 33), which permitted this parameter to patient was prescribed oral zinc sulfate (7H2O) 50-200 remain almost identical to that of the pretreatment level mg three times per day. Despite this the patients were relieved of symp induced a significant reduction on serum copper levels in toms. This may indicate that copper in our cases had no few days recurrence of symptoms may soon be relation to genesis of psoriasis nor to its treatment. Brit Med J, occurred in a series of over two thousand patients on this 11:591-594, 1953. Under these precautions in no case an chemistry of the parakerotitik lesion of swine. J Invest Derm, undue rise of serum zinc or copper to toxic levels was 48:521-530, 1967. It is important to note that the serum zinc levels were Vestu Derm Vener, 40:14-18, 1966. Br J Derma other cases however when the serum zinc content rose to tol, 84:178, 1971. N with Grenz ray or topical corticosteroid combined with Grenz Engl J Med, 301:535, 1979. Roenigk H, Farber E, Storrs F, et al: Photochemother Valdimarsson H, Fry L: Long term cyclosporin for psoriasis. Kekki M, Koskelo P, Lassus A: Serum ceruloplasmin Am Acad Dermatol, 7:758-762, 1982. Generally chronic skin diseases typically arent curable, but they can be managed using drugs. The prescribed synthetic drugs for the treatment of psoriasis are associated with severe side effects, thus, researchers around the globe are searching for new, effective, and safer drugs from natural resources. Virtually all cultures worldwide have relied historically, or continue to rely on medicinal plants for Skin diseases. The objective of this paper is to list out the beneficial effects of certain medicinal plants for treating skin diseases. The present review has been prepared with an objective to compile exhaustive literature on pharmacological reports on antipsoriatic plants, plant products, and formulations. Plants selected for the present review are having medicinally significant value and many of them possess active phytochemical constituents. Keywords: Psoriasis, Topical treatment, Corticosteroids, Vitamin D Analogs, Tazarotene and Coal tar. Psoriasis is a Psoriasis is a long-term condition, psoriasis is not infectious, common skin condition which can be itchy and painful; but psoriasis can affect all areas of the skin. Psoriasis can range from being a very new skin cells more quickly than normal and these build up on mild to a very serious condition. This is related to your immune cure for psoriasis, but it can be well controlled by using a response, which is the way in which your body fights diseases variety of treatments. In psoriasis, your immune system triggers There are different types of Psoriasis [2] a reaction even though there is no infection or wound to heal. Pustular psoriasis prescribed synthetic drugs for the treatment of psoriasis are 4. Inverse psoriasis associated with severe side effects, thus, researchers around 5. These patients can often be treated successfully with topical therapies, including corticosteroids, vitamin D analogs, tazarotene and 40 calcineurin inhibitors. Tazarotene is as effective as topical corticosteroids in alleviating symptoms of Figure 1: Comparison of Topical Therapies for Psoriasis psoriasis, but it is associated with a longer disease-free interval. Botanical name Family name Common name & Local name Plant parts used 1 Aloe vera Liliaceae Aloes, Kathalai Leaf 2 Alpinia galanga Zingiberaceae Thai Ginger, akkulati Rhizome 3 Angelica sinensis Apiaceae Chinese angelica Root 4 Andrographis nallamalayanna Acanthaceae Echinacea, Siriyaa Nangai/Nila Vembu Whole plant 5 Annona squamosa Annonaceae Sugar Apple, Custardapple Sitapalam Rhizome and leaf 6 Argemone mexicana L. Meliaceae Neem, Veppam Leaves, bark and stem 8 Caesalpinia bonducella Caesalpiniaceae Fever nut, Kalichchikkai Leaves 9 Calendula officinalis Compositae Marigold, Thulukka Saamanthi Flowers 10 Capsicum annum Solaneceae Cayenne, Milagai Leaves 12 Cassia fistula L. Apiaceae Indian Pennywort Vallarai Whole plant 15 Crotalaria juncea leguminosae Sunn hemp,Vakkunnar Seeds 16 Curcuma longa L. Zingiberaceae Turmeric, Manjal Rhizome 17 Givotia rottleriformis Euphorbiaceae White Catamaran Tree puttali bark 18 Leucas aspera Lamiaceae Common leucas, Thumbai Aerial parts 19 Matricaria recutita Asteracea Chamomile, Mookuthi Poo Flowers 20 Melaleuca alternifolia Myrtaceae Tea tee oil 21 Momordica charantia L. Cucurbitaceae Bitter Gourd, iraca-valli Pavai Seeds 22 Nigella sativa Ranunculaceae Black cumin, Karunjiragam Seeds 23 Pongamia pinnata (L. Rubiaceae Indian Madder, Manjitti 27 Silibum marianum Asteraceae Milk thistle, vishnu kranti 28 Smilax china Smilacaceae China Root Parangichekkai Rhizome 29 Thespesia populnea Malvaceae Indian tulip tree Puvarasu Bark 30 Tribulus terristris Zygophyllaceae Puncture Vine, palleru-mullu 31 Ulmus rubra Ulmaceae slippery elm Barks 32 Urgenia indica Liliaceae Indian squil, l Narivengayam Bulbs 33 Vitex glabarata Lamiaceae Chastetree Leaves 34 Wrightia tinctoria L. Aloe vera the alternate, pinnate leaves are 20-40 cm long, with 20-31 the leaves are thick and fleshy, green to grey-green, with medium to dark green leaflets about 3-8 cm long. The stem some varieties showing white flecks on their upper and lower bark is burnt and ash is applied topically on boils. The margin of the leaf is serrated and has of leaves is used to bath for the treatment of body infection. The active agents have shown considerable Its decoction is also taken orally for the treatment of the analgesic, antipruritic, wound healing and anti-inflammatory same. The seed oil is used externally to kill lice and to treat properties, thus justifying consideration of Aloe vera as an dandruff. Chanachai et al (2009) reported the plant in few remote villages in Kolli Hills, Nammakal District of Alpinia galanga, Curcuma longa and Annona squamosa for Tamilnadu, India. Its seeds are used in skin diseases, leprosy their anti-psoriatic effect [20] and inflammation a number of cassane furanoditerpenes 3. Angelica sinensis were reported to be isolated from different parts of the Angelicas are biennials or short-lived perennials belonging to plant [27-33] the Apiaceae family. Calendula officinalis three-sectioned leaves, borne on clasping leafstalks, which Calendula officinalis is a short-lived aromatic herbaceous may be 2 to 3 feet tall. Calendula officinalis 22, 23] (Family: Compositae) are some of the very common Indian 4. Andrographis nallamalayanna herb having various medicinal properties for the treatment of the plant is being used in folklore system of medicine to treat different kind of disease, viz. Annona squamosa been reported for their usefulness in the form of decoctions, the leaves are thin, oblong while the flowers are greenish infusions and tinctures in traditional system of medicines for yellow. Capsicum annum Curcuma longa and Annona squamosa for their anti-psoriatic A large perennial shrub, the single flowers are an off-white effect. The Mexican Prickly Poppy is a prickly, hairless, branching herb herb contains a substance known as capsaicin, which relieves with yellow juice and showy Leaves are thistle like, stem pain and itching associated with psoriasis. The leaves applied externally effective in plaque Psoriasis [43, 44, paste of seeds is applied topically on itching. The latex is this native of India, commonly known as Amaltaas, It has applied externally in cracks on feet. The latex along with showy racemes, up to 2" long, with bright, yellow, fragrant cow milk is placed in copper pot for 3 days and applied flowers. Each leaf Common Leucas is an erect and diffusely branched annual has three pairs of leaflets that are opposite, ovate, oblong herb. Whorls are large, terminal known as Charota, Chakunda and Sickle senna locally, has and axillary, about 2. Crotalaria juncea A tall shrub or small tree up to 7 m high with a bushy crown Sunn hemp is a rapid growing crop that is used for fiber and papery bark. Used In the treatment of acne, high with elliptical lanceolate leaves and yellow terminal dandruff and cold sores, tea tree oil can produce allergic flowers. Momordica charantia distributed in the tropical and subtropical region of India, Bitter Gourd is a herbaceous, tendril-bearing vine, growing Nepal, Sri Lanka, and Southern Africa. It bears simple, alternate leaves 4-12 cm across, blood purifier, abortificient, astringent, demulcent, emetic, with 3-7 deeply separated lobes. Used in the form of purgative and in the treatment of anaemia, impetigo, decoctions and infusions to treat bacterial infections and also menorrhagia and psoriasis [56, 57, 58, 59] claimed to be an effective against variety of skin conditions 15. Curcuma longa like psoriasis, acne, wounds [69] Turmeric is a rhizomatous herb, the plant grows to a height Momordica charantia (Family: Cucurbitaceae) are some of the of 3-5 ft.
Siegrist streaks are flecks which are arranged lineraly along the choroidal vessels antibiotics for dogs cost order 200 mg doxycycline mastercard. Keith Wagner and Barker (1939) Keith antibiotic erythromycin purchase doxycycline 200 mg, Wagner and Barker (1939) have classified hypertensive retinopathy into four grades on the basis of ophthalmoscopic characteristics bacteria vs archaea order cheapest doxycycline and doxycycline. It correlates directly with the degree of hypertension and inversely with the prognosis for survival of patients antibiotics for dogs eye order 100 mg doxycycline mastercard. Grade 1 Mild to moderate narrowing or sclerosis of the retinal arterioles is present antimicrobial step 1 buy doxycycline 100mg without a prescription. These patients have benign essential hypertension with adequate cardiorenal function bacteria 4 billion years ago order doxycycline 200mg fast delivery. Cotton wool or soft exudates consisting of fibrin and protein are scattered all over the fundus. Macular star is formed due to accumulation of hard exudates in the outer plexiform layer. Grade 2 Severe narrowing with localized irregular constriction of the arterioles. Grade 3 Narrowing and focal irregularities of arterioles, retinal haemorrhage and exudates. Grade 4 All changes in grade 3 along with neuroretinal oedema, and / or papilloedema. Arteriolo-sclerotic features these changes develop if the hypertension is present over a period of many years, and are mainly seen in aged individual. The Retina 315 Clinical Types Clinically, hypertensive retinopathy may occur in four forms as follows: 1. Energetic treatment with antihypertensive drugs results in remarkable improvement of the fundus picture. Control of high blood pressure with rest, sedation, salt restriction, diuretics and antihypertensive drugs is a must. Termination of pregnancy is advised in cases of severe retinopathy not responding to treatment. With increase in life expectancy in diabetic patients, the incidence of diabetic retinopathy has increased. It affects young or old alike, for it is the diabetic age and not the actual age that is important. Presence of retinopathy is not related to the prognosis of diabetes and expectancy of life. Predisposing Factors the following factors influence the occurrence of diabetic retinopathy, 1. Approximately 50% of diabetic patients develop retinopathy after 10 years and about 80% after 15 years. Essentially, it is a microangiopathy affecting retinal precapillary anterioles, capillaries and venules. There is loss of intramural pericytes which are normally persent in the basement layers. Microangiopathy results in microvascular occlusion, microaneurysm, capillary leakage and haemorrhages. Retinal hypoxia in turn causes formation of hard exudates, arteriovenous shunt formation and neovascularisation. They look like cluster of grapes at the end of vascular twigs particularly in the macular area while doing fluorescein angiography. They are seen on the venous side of capillary net work at the inner nuclear layer. They are white or yellow coloured, waxy looking patches of exudates containing hyaline and lipid with clear-cut and often serrated margins. Fluorescein angiographically diabetic maculopathy can be classified into four types: a. Advanced Diabetic Eye Disease It is the end result of uncontrolled proliferative diabetic retinopathy. There is marked visual loss due to neovascular glaucoma, vitreous haemorrhage and tractional retinal detachment. Increased risk of visual loss v Neovascularization Vitreous Secondary Maculopathy Cataract haemorrhage glaucoma the Retina 321 Prognosis It is usually bad. There is increased risk of visual loss over 2 years period in cases of vitreous haemorrhage, neovascularisation, secondary glaucoma, cataract formation and maculopathy. Fluorescein angiography and coloured fundus photographs should be taken as a record. Adequate medical control with low fat and anti diabetic drugs reduces the ocular and systemic complications. It reduces retinal ischaemia which in turn prevents further neovascularisation and vitreous haemorrhage. Focal argon laser burns are applied to individual microvascular formations in the centre of the hard exudate ring in focal exudative maculopathy. It is the most common cause of permanent central visual loss in the elderly in developed countries. Etiology It is caused by sclerosis of the arteries which nourish the retina depriving it of oxygen and other nutrients. Predisposing factors include heredity, age, nutrition, smoking, hypertension and excessive exposure to sunlight. Drusen looks like small, bright, sharply defined circular points lying below the retinal vessels. It appears as a recessive trait and usually occurs due to consanguinity of the parents. There is gradual constriction of the visual fields resulting in small central tubular vision. The retinal veins, never the arteries, may have a sheath of pigment for part of their course. Laurence-Moon-Biedl syndrome Obesity, Hypogenitalism, Mental defect, Polydactyly, 1. It is due to the proliferation of neural cells which have failed to evolve normally. Occasionally, it may remain quiescent and manifest in the 5th or 6th year or even later. Chromosomal abnormalities such as deletion of long arm of chromosome-13 and trisomy-21 may be present. High power microscopic examination shows two different types of cellular characteristics. Poorly differentiated, small to medium sized round cells with large hyperchromatic nuclei and scanty cytoplasm along with necrosis. This type of cell arrangement can also be seen in neuroblastoma and medulloepithelioma. It is due to reflection of light from the yellow-white mass in the retrolental area. Pseudohypopyon with esotropia (convergent squint) may be the presenting clinical feature. The second eye may show a larger retinal tumour mass surrounded by numerous punctate satellites. Differential Diagnosis In all cases atropine is instilled and thorough fundus examination of both eyes should be done under general anaesthesia to rule out bilateral involvement. Inflammatory deposits in the vitreous following a plastic cyclitis or choroiditis. Congenital defects, due to persistent hyperplastic vitreous at the back of the lens. Lactic dehydrogenase and phosphoglucose isomerase enzyme levels are raised in the aqueous humor.
O Antibiotic eyedrops for first aid treatment of injuries infection ios trusted 100mg doxycycline, sterile eye compresses antibiotics for uti in cats doxycycline 100mg with amex, and a 1cm adhesive bandage for protective bandaging bacteria without cell wall buy doxycycline american express. An ophthalmologist should be consulted following any emergency treatment of eye injuries virus 20 furaffinity order doxycycline without prescription. Many eye disorders are hereditary or of higher incidence in members of the same family antibiotic for skin infection generic 200 mg doxycycline with visa. Examples include refractive errors antibiotic resistance ethics generic doxycycline 100 mg on line, stra bismus, cataract, glaucoma, retinal detachment, and retinal dystrophy. As ocular changes may be related to systemic disorders, this possibility must be explored. Conditions affecting the eyes include diabetes mellitus, hypertension, infectious diseases, rheumatic disorders, skin diseases, and surgery. Eye disorders such as corticosteroid-induced glaucoma, corticosteroid-induced cataract, and chloroquine-induced maculopathy can occur as a result of treatment with medications such as steroids, chloroquine, Amiodarone, Myambutol, or chlorpromazine (see table in Appendix). The examiner should inquire about corrective lenses, strabismus or amblyopia, posttraumatic conditions, and surgery or eye inflammation. Does the patient have impaired vision, pain, redness of the eye, or double vision One eye is covered with a piece of paper or the palm of the hand placed lightly over the eye. The fingers should not be used to cover the eye because the patient will be able to see between them. The general practitioner or student can perform an approximate test of visual acuity. The patient is first asked to identify certain visual symbols referredtoasoptotypes(seeFig. These visual symbols are designed so that optotypes of a cer tain size can barely be resolved by the normal eye at a specified distance (this standard distance is specified in meters next to the respective symbol). The sharpness of vision measured is expressed as a fraction: Examining visual acuity. A normal-sighted person would be able to discern the 4 at a distance of 50 meters or 200 feet (standard distance). The ophthalmologist tests visual acuity after determining objective refraction using the integral lens system of a Phoroptor, or a box of individual lenses and an image projector that projects the visual symbols at a defined distance in front of the eye. Visual acuity is automatically calculated from the fixed actual distance and is displayed as a decimal value. Plus lenses (convex lenses) are used for farsightedness (hyperopia or hypermetropia), minus lenses (concave lenses) for nearsightedness (myopia), and cylindrical lenses for astigmatism. If the patient cannot discern the symbols on the eye chart at a distance of 5 meters (20 feet), the examiner shows the patient the chart at a distance of 1 meter or 3 feet (both the ophthalmologist and the general practitioner use eye charts for this examination). If the patient is still unable to discern any symbols, the examiner has the patient count fingers, discern the direction of hand motion, and discern the direction of a point light source. This allows the examiner to diagnose strabismus, paralysis of ocular muscles, and gaze paresis. Evaluating the six cardinal directions of gaze (right, left, upper right, lower right, upper left, lower left) is sufficient when examining paralysis of the one of the six extraocular muscles. The motion impairment of the eye resulting from paralysis of an ocular muscle will be most evident in these positions. Only one of the rectus muscles is involved in each of the left and rightpositionsofgaze(lateralormedialrectusmuscle). If the corneal reflection is not in the center of the pupil in one eye, then a tropia is present in that eye. If tropia is present in a newborn with extremely poor vision, the baby will not tolerate the good eye being covered. Stenosis of the nasolacrimal duct produces a pool of tears in the medial angle of the eye with lacrimation (epiphora). In inflammation of the lacrimal sac, pressure on the nasolacrimal sac frequently causes a reflux of mucus or pus from the inferior punctum. Patency of the nasolacrimal duct is tested by instilling a 10% fluorescein solution in the conjunctival sac of the eye. If the dye is present in nasal mucus expelled into paper tissue after two minutes, the lacrimal duct is open (see also p. Due to the danger of infection, any probing or irrigation of the nasolacrimal duct should be performed only by an ophthalmologist. The bulbar conjunctiva is directly visible between the eyelids; the palpebral conjunctiva can only be examined by everting the upper or lower eyelid. The examiner should be alert to any reddening, secretion, thickening, scars, or foreign bodies. The patient looks up while the examiner pulls the eyelid downward close to the anterior margin. The patient looks up while the ex aminer pulls the eyelid downward close to the ante rior margin. The patient should repeatedly be told to relax and to avoid tightly shutting the opposite eye. The examiner grasps the eyelashes of the upper eyelid between the thumb and forefinger and everts the eyelid against a glass rod or swab used as a fulcrum. Eversion should be performed with a quick levering motion while applying slight traction. The examiner places a swab superior to the tarsal region of the upper eyelid, grasps the eyelashes of the upper eyelid between the thumb and forefinger, and everts the eyelid using the swab as a fulcrum. To expose the superior fornix, the upper eyelid is fully everted around a Desmarres eyelid retractor. This method is used solely by the ophthalmologist and is only discussed here for the sake of completeness. This eversion technique is required to remove for eign bodies or lost contact lenses from the superior fornix or to clean the conjunctiva of lime particles in a chemical injury with lime. Examination of the upper eyelid and superior fornix (full eversion with retractor). In contrast to simple eversion, this procedure allows examination of the superior fornix in addition to the palpebral conjunctiva. In these cases, the spasm should first be eliminated by instilling a topical anesthetic such as oxy buprocaine hydrochloride eyedrops. Epithelial defects, which are also very painful, will take on an intense green color after application of fluorescein dye; corneal infiltrates and scars are grayish white. Sensitivity is evaluated bilaterally to detect possible differences in the reaction of both eyes. The examiner holds the upper eyelid to prevent reflexive closing and touches the cornea anteriorly. Decreased sensitivity can provide information about trigeminal or facial neuropathy, or may be a sign of a viral infection of the cornea. The patient looks straight ahead while the examiner holds the upper eyelid and touches the cornea anteriorly. In a cham ber of normal depth, the iris can be well illuminated by a lateral light source. The pupillary dilation should be avoided in patients with shallow ante rior chambers because of the risk of precipitating a glaucoma attack. Dilation of the pupil with a mydriatic is contraindicated in patients with a shallow anterior chamber due to the risk of precipitating angle closure glaucoma. Direct illumination will produce a red reflection of the fundus if the lens is clear and gray shadows if lens opacities are present. The examiner then illuminates the eye laterally with a focused light held as close to the eye as possible and inspects the eye through a +14 diopter loupe (see. This examination permits better evaluation of changes in the conjunctiva, cornea, and anterior chamber. With severe opacification of the lens, a gray coloration will be vis ible in the pupillary plane. Each vascular structure should be of uni form diameter, and there should be no vascular constriction where vessels overlap. Younger patients will have a foveal and macular light reflex, and the retina will have a reddish color (see. The examiner moves an object such as a pen, cotton swab, or finger from the periphery toward the midline in all four quadrants (in the superior and infe rior nasal fields and superior and inferior temporal fields). A patient with a normal field of vision will see the object at the same time as the examiner; a patient with an abnormal or restricted field of vision will see the object later than the examiner. It can be used to diagnose a severely restricted field of vision such as homonymous hemianopsia or quadrant anopsia. The examiner moves a pen from the periphery toward the midline in all four quadrants in the nasal and temporal fields and in the superior and inferior fields. Slight increases in intraocular pressure such as occur in chronic glau coma will not be palpable. One drop or strip of ointment approximately 1cm long should be administered laterally to the inferior conjunctival sac. To avoid injury to the eye, drops should be administered with the patient supine. Eye ointment should not be administered following ocular trauma as this may complicate subsequent examination or surgery. Dilation of the pupils with a mydriatic in unconscious patients should be avoided as this complicates neurologic examination. A sterile swab or commercially available bandage (two oval layers of bandage material with a layer cotton between them) may be used. Strong mechanical, optical, and acoustic stimuli (such as a foreign body, blinding light, or sudden loud noise) automatically elicit an eye closing reflex. Structure of the eyelids: the eyelids consist of superficial and deep layers. The tarsal muscle is supplied by the sympathetic nervous system and regulates the width of the palpebral fissure. High sympathetic tone contracts the tarsal muscle and widens the palpebral fissure; low sympathetic tone relaxes the tarsal muscle and narrows the palpebral fissure. Every time the eye blinks, it acts like a windshield wiper and uniformly distributes glandular secretions and tears over the conjunctiva and cornea. Orbicularis oculi muscle Orbital septum Orbital fat Levator palpebrae muscle Accessory lacrimal gland Superior M. Thedeeplayerconsists of the tarsal plate, tarsal muscle, palpebral conjunctiva, and meibomian glands. Their function is to prevent the escape of tear fluid past the margins of the eyelids. On the upper eyelid, approximately 150 eyelashes are arranged in three or four rows; on the lower eyelid there are about 75 in two rows. Like the eyebrows, the eyelashes help prevent dust and sweat from entering the eye. The orbital septum is located between the tarsal plate and the margin of the orbit. It is a membranous sheet of connective tissue attached to the margin of the orbit that retains the orbital fat. Bilateral inspection of the eyelids includes the following aspects: O Eyelid position: Normally the margins of the eyelids are in contact with the eyeball and the puncta are submerged in the lacus lacrimalis. O Width of the palpebral fissure: When the eye is open and looking straight ahead, the upper lid should cover the superior margin of the cornea by about 2mm. Occasionally a thin strip of sclera will be visible between the cornea and the margin of the lower lid. Varying widths of the gaps between the eyelids may be a sign of protrusion of the eyeball, enophthal mos, or eyeballs of varying size (Table 2. O Skin of the eyelid: the skin of the eyelid is thin with only a slight amount of subcutaneous fatty tissue. Allergic reaction and inflammation can rapidly cause extensive edema and swelling. In older patients, the skin of the upper eyelid may become increasingly flaccid (cutis laxa senilis). Occa sionally it can even hang down over the eyelashes and restrict the field of vision (dermatochalasis or blepharochalasis). The normal palpebral conjunctiva is smooth and shiny without any scar strictures or papilliform projections. Colobomas are rare defects resulting from a reduction malformation (defective closure of the optic cup). Diagnostic considerations: the disorder is often accompanied by additional deformities such as dermoid cysts or a microphthalmos. Depending on the extent of the coloboma, desiccation symptoms on the conjunctiva and cornea with incipient ulceration may arise from the lack of regular and uniform moisten ing of the conjunctiva and cornea. Treatment: Defects are closed by direct approximation or plastic surgery with a skin flap. The nasal bridge becomes more pro nounced as the child grows, and most epicanthal folds disappear by the age of four. Blepharophimosis is a rare disorder that is either congenital or acquired (for example, from scar contracture or aging). As long as the center of the pupil remains unobstructed despite the decreased size of the palpebral fissure, surgical enlargement of the palpebral fissure (by canthotomy or plastic surgery) has a purely cosmetic purpose. Usually, the partial or total fusion between the upper and lower eyelids will be bilateral, and the palpebral fissure will be partially or completely occluded as a result. The following forms are differentiated according to their origin (see also Etiology): O Congenital ptosis.
Cheap doxycycline. See C. diff Campaign.
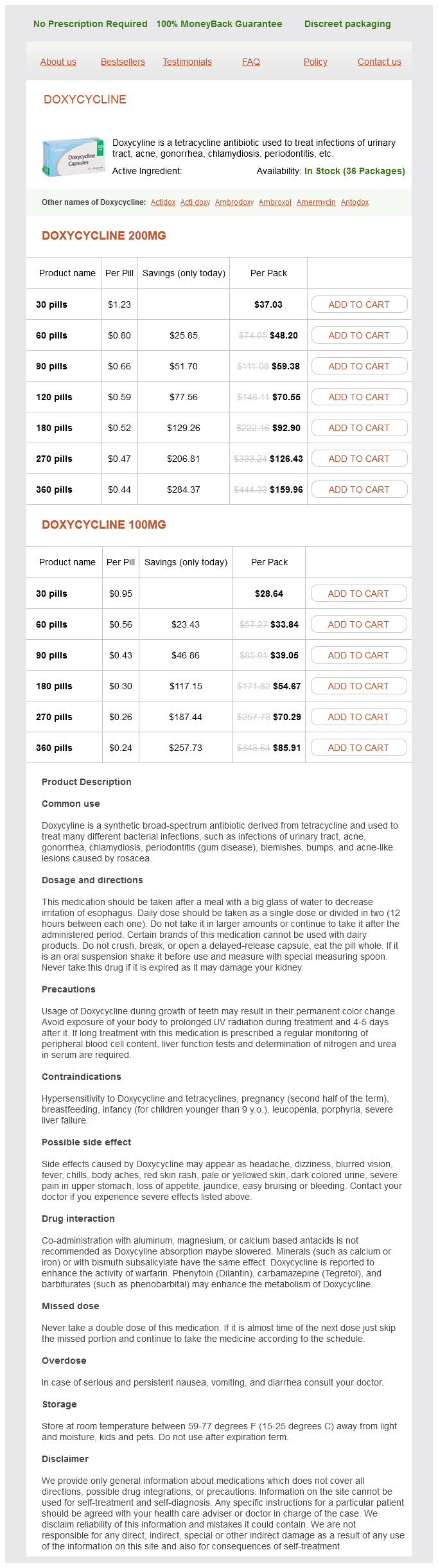
Digital subtraction angiography in a patient with isolated thrombosis of the right inferior anastomotic vein of Labbe (right) bacteria facts for kids order doxycycline visa, in contrast to physiological imaging of the cerebral vein findings of the contralateral hemisphere (left) xanthone antimicrobial generic doxycycline 200 mg free shipping. Impaired consciousness and cerebral hemorrhage on Anticardiolipin IgG and IgM antibodies admission are associated with a poor outcome virus del papiloma humano cheap doxycycline 200 mg visa. The first study was ter the advantage of dose-adjusted intravenous heparin minated after inclusion of 10 patients in each group bacteria lesson plan purchase 100 mg doxycycline amex, therapy bacteria viruses buy doxycycline now, particularly in critical ill patients bacterial 8 letters doxycycline 100 mg discount, may be the as an interim analysis documented a beneficial effect fact that the activated partial thromboplastin time of heparin treatment on morbidity and mortality. Both studies were tory effect of heparin may be immediately antagonized criticized for inadequately small sample size [8]or with protamin, while such an antidote is not available baseline imbalance favoring the placebo group [6]. Immediate anticoagulation is recommended, even A meta-analysis of the studies on immediate anti in the presence of hemorrhagic venous infarcts. Chapter 11: Cerebral venous thrombosis According to current guidelines [1], oral anti complications. Acetylsalicylic Thrombolysis acid should be avoided, as the patients bleeding risk may be increased due to the concomitant anticoagu Despite immediate anticoagulation, some patients lation treatment. Severe headache may require treat show a distinct deterioration of their clinical condi ment with opioids, but dose titration should be tion, and this risk seems to be especially high in performed cautiously in order to avoid over-sedation. A potential publication bias in the For the treatment of headaches, paracetamol current published work has been assumed, with pos should be preferred over acetylsalicylic acid 173 sible under-reporting of cases with poor outcome and because of the patients bleeding risk. One study identified focal sensory deficits rapid improvement of headache and visual function. A hemorrhagic lesion diuretic drugs are not as quickly eliminated from in the acute brain scan was the strongest predictor of the intracerebral circulation as in other conditions post-acute seizures [22]. Osmodiuretics common in patients with early symptomatic seizures may thus reduce venous drainage and should there than in those patients with none. Increased intracranial pressure in most cases Epileptic seizures should be treated with paren responds to improved venous drainage after anti terally administered antiepileptic drugs (phenytoin, coagulation. Chapter 11: Cerebral venous thrombosis occluded cerebral veins, but also in order to prevent Infectious thrombosis the recurrence of intra or extracerebral thrombosis. Antithrombo ingly favorable, with an overall death or dependency tic prophylaxis during pregnancy is probably unneces rate of about 15% [2]. However, women on vitamin K antagonists nancy, deep venous system thrombosis, intracranial should be advised not to become pregnant because of hemorrhage, coma upon admission, age and male sex. The main causes of acute death are transtentorial herniation secondary to a large hemorrhagic lesion, multiple brain lesions or diffuse Special aspects brain edema. Fatalities after the acute phase are predominantly eclampsia, gestational or chronic diabetes mellitus). A significant number of Recurrence of cerebral venous children are left with a considerable impairment thrombosis (motor or cognitive deficits, epilepsy). Future developments Treatment of bacterial infections with broad antibiotics and surgery. Open questions con Treatment of epileptic seizures with parenterally cern many of our current management decisions, administered antiepileptic drugs (phenytoin, such as the role of local or systemic thrombolysis, valproic acid, levetiracetam). Prognosis of the most common and frequently the first cerebral vein and dural sinus thrombosis. Martins and Lara Caeiro Cognitive functions are related to our ability to build lesions are circumscribed, the conceptual representa an internal representation of the world, the concep tion system is not affected and these patients are not tual representation system, based on a large-scale demented. Although tion, organized according to their specific processing these tests are also included in brief exams of cogni capacities. In fact, language impairment will affect typed, since it follows the distribution of the vascular the majority of cognitive functions and needs to be territories. However, in the hyperacute stage symp ruled out before proceeding to the assessment of toms are likely to be amplified by additional regions orientation, memory or executive functions. It is also a rough plasticity mechanisms make neuroanatomical corre measure of aphasia severity. Presented objects should be venous thrombosis the pattern of cognitive defects is common and easily recognized (spoon, comb, spec less stereotyped due to the variability of lesion local tacles, pencil, wristwatch), to make the task specific ization, size and number, or particular pathogenic for aphasia and not sensitive to cultural factors or mechanisms that may cause diffuse impairment. Patients responses vary from pauses (word In this chapter we will present the most common finding difficulties), tip-of-the tongue phenomenon, cognitive and neurobehavioral deficits secondary to paraphasias, the use of supraordinal responses (fruit stroke, according to symptom presentation. There are rare patients who suffer from a selective naming difficulty affecting a single category of names Language disorders (category-specific impairments), such as living Language disorders, or aphasia, occur following peri entities, actions but not objects, or proper names sylvian lesions (middle cerebral artery territory) of the but not common names. These unusual cases demon left hemisphere and have a marked impact on the strate that the mental lexicon/semantic system is 178 individual quality of life, autonomy and the ability organized by the functional or physical properties of to return to work or previous activities. Chapter 12: Behavioral neurology of stroke the analysis of speech is performed during spon with posterior temporal lesions, while inferior frontal/ taneous or induced conversation (asking patients to opercular lesions tend to impair the understanding of tell you an episode or to describe a picture). To make this sounds that do not belong to the lexicon) and sen classification easy the listener should try to ignore the tences, to evaluate the ability to decode, retain briefly content of speech (as if listening to a foreign lan in memory and reproduce phonemes (speech guage) and concentrate on the effort, speech rate sounds). Transcortical aphasias are characterized by and the number and duration of pauses. Fluent a disproportionate capacity to repeat, compared to speech sounds normal as opposed to nonfluent other language abilities. Verbal auditory comprehension is tested through In conduction aphasia, in contrast, patients have out simple verbal commands (close your eyes, raise standing difficulty in repeating pseudowords or even your arm, etc. Effective language recovery, in adults, depends Speech fluency mostly upon the reorganization of the intact areas of Fluent Non-fluent the left hemisphere in the neighborhood of the lesion [3]. Normal output Slow output Four cardinal tests are useful for a bedside evalu ation of aphasia and to localize lesions, since they (words/minute) Single words have neuroanatomical correlates: (1) confrontation Normal phrase Telegraphic sentences naming; (2) analysis of speech (fluent and nonflu length ent); (3) verbal auditory comprehension; (4) repeti tion of words, pseudowords and sentences. Effortless Effortful Language should be evaluated before cognitive No pauses Hesitations, pauses, interruptions assessment. Normal prosody Loss of prosody Certain brain lesions may impair the ability to Sounds normal Sounds atypical read (alexia or acquired dyslexia) or to write (agra phia/dysgraphia). In contrast, in surface the study of patients with reading or writing dyslexia patients can read aloud regular words and disorders has contributed to the understanding of pseudowords (because they can convert letters, writ the cognitive processes subserving those abilities and ten graphemes, to their corresponding sound), but to the building of theoretical models of them. They have difficulty reading irregular words or accessing have shown that there are separate pathways to pro their meaning. These opposite types of impairment cess particular categories of words (regular vs. This information has been incorpor and a step-by-step conversion that is useful for read ated into the assessment and classification of these ing new or infrequent words. Likewise, in central agraphias, the writing impair Alexia and agraphia can be classified as central or ment is similar across different output modalities peripheral, depending on whether the impairment (handwriting, spelling or typing) and can be of a affects the central processing or the afferent or effer deep type (phonological dysgraphia) with preserved ent pathways. In this syndrome, patients can read through the tactile There are also cases whose defect involves the graph and auditory modalities (read a word that is spelled emic buffer (a short-term memory device that aloud to them), showing that the central processing is enables the writer to keep the word on line as it is intact. They can also write to dictation or sponta being written in real time), which is characterized by a neously. However, they cannot associate visually pre particular difficulty writing long words. In contrast, sented written words with their sound or meanings peripheral agraphia is a selective damage in the selec (cannot read). This syndrome results from a discon tion or the act of drawing letters (during handwriting) nection between the visual areas and the word form that can be overcome by typing or the use of ana area, due to left temporo-occipital infarcts involving grams and is associated with normal spelling. Deep forms of dyslexia and dysgraphia are associ In central dyslexias, the impairment is indepen ated with large left hemisphere strokes [5], while dent of the presentation modality (visual, auditory or surface types result from more limited lesions. It is tactile) and therefore also involves writing and spell possible that reading and writing/spelling rely on ing. Declarative Alexia and agraphia are commonly found in apha Semantic sia, but may occur in isolation following lesions of the left hemisphere. Alexia can be classified as Episodic central and peripheral, and as with deep and with surface Implicit types. Neglect has a negative impact on the hemispace contralateral to a brain lesion, usu daily living activities and on functional recovery, ally of the right hemisphere. Selective attention relies on a large network Memory disturbances involving the anterior cingulate gyrus (responsible Memory is not a unitary function. It consists of five for its motivational aspects), frontal-parietal and independent systems and involves three processes superior temporal regions (afferent and intentional/ (encoding, storing/consolidation and retrieval). Both exploratory aspects) as well as subcortical structures, depend on specific neural networks that may dissoci such as the thalamus and the striatum. It may be evident memory traces (fractions of seconds, seconds or for in different types of space: in the personal space life), content (explicit knowledge or motor routines) (forgetting to dress, groom the left side of the body), and access to consciousness (explicit or implicit). It may be present spontaneously or during retrieving information that was already stored). In its most severe form it comprises ano result from posterior cerebral artery, posterior com sognosia or denial of illness/impairment and a loss of municating artery, anterior and posterior choroidal identification of body parts as belonging to the self. Infarcts in the terri performed in the peri-personal space and require the tories of the two last arteries can also be secondary to patient to draw, copy or cross out lines or other stimuli subarachnoid hemorrhage and its complications and (cancellation tasks) or to read or write. A qualitative to the surgical and less often to the endovascular analysis of the defect allow us to further classify the treatment of aneurysms located in these arteries. Anterolateral and medial thalamic hemor or partial recovery of memory disturbances can be rhages, caudate and intraventricular hemorrhages and expected. Bilateral infarcts produce global and severe venous infarcts due to thrombosis of the deep venous amnesia and a persistent deficit, with slow and limited system also produce memory defects. In thalamic amnesia confabulations, A quarter of posterior cerebral artery infarcts intrusions and perseveration are frequent. These ibility, alternating good and poor performance and amnestic strokes usually have mesial temporal better performance on first attempts are also involvement and the damage extends beyond the characteristic. Confabulations appear to be hippocampal atrophy was found on neuroimaging more likely if there is a dual lesion (temporo-occipital studies in subarachnoid hemorrhage survivors [14]. Amnesia following rupture of anterior communi In thalamic infarcts [12], memory defects cating aneurysms is characterized by a severe antero (Table 12. Amnesia is related to damage to the anterior cingu Left thalamic infarcts can produce pure amnesia in lum, subcalosal area and basal forebrain. Memory error contexts are associated with ventromedial pre disturbances are more frequent and severe after left frontal cortex damage, but for spontaneous confabu 182 than after right thalamic infarcts. Right thalamic lations to occur there must be additional orbitofrontal infarcts cause visual and/or visuospatial amnesia. The brain has a mechanism to distinguish Chapter 12: Behavioral neurology of stroke mental activity representing ongoing perception of Table 12. Confabulations can be traced to fragments of previous actual experi Interview ences. Confabulators confuse ongoing reality with the Frontal Behavioral Inventory past because they fail to suppress evoked memories that do not pertain to the current reality. Frontal Assessment Battery at bedside Classification of memory systems depends upon Specific tests duration of memory traces, content, and access to consciousness. Stroke in function produces three distinct clinical syndromes some specific locations can cause executive deficits, composed respectively of executive deficits, uninhib disinhibition or apathy. Executive difficulties mani artery infarcts with frontal lobe or striatocapsular fest as difficulty deciding, leaving decisions to proxy involvement, uni or bilateral anterior cerebral artery and being stubborn or rigid. Examples of uninhibited infarcts, anterior or paramedian thalamic infarcts, behavior include inappropriate familiarity, being dis striatocapsular, thalamic, intraventricular or frontal tractible and shouting when constrained and manipu intracerebral hemorrhages, subarachnoid hemorrhage lation or utilization behavior. Recent models propose due to rupture of anterior communicating artery four main executive functions: dual task coordination, aneurysms and thrombosis of the saggital sinus or of switch retrieval, selective attention and holding and the deep venous system. Visual agnosia the human brain has two parallel visual systems: a According to the type of visual stimuli ventral occipito-temporal stream, whose main func Visual agnosia for tion is the recognition of visual stimuli (the what Letters and words system) and a dorsal occipito-parietal stream, whose main function is the spatial localization of visual Other symbols stimuli (the where system) [20]. Specific classes of objects Visual agnosias are disorders of visual recognition Faces and are one of the clinical manifestations of posterior Locations cerebral artery infarcts and occipito-temporal hemor rhages. Agnosias can be seen in patients improving According to the functional processes involved from cortical blindness. Visual agnosias can be classi Apperceptive visual agnosia fied following the type of stimuli that is defectively Form agnosia recognized or following the impaired functional step in the processing of information from the visual Integrative agnosia system to the semantic and the language systems Associative visual agnosia (Table 12. Disconnection or loss of semantic access Apperceptive visual object agnosia is characterized by the presence of perceptual defects in visuopercep Loss of semantic knowledge tive tasks and a defective perception of elementary perceptual features (color, shape, contour, bright ness). Patients with this type of agnosia apperceptive visual agnosia is visual matching errors show not only intact naming in other modalities when trying to match identical visual stimuli. They perform better with real objects than object in multiple-choice tasks and can sort objects by with drawings. Patients or pantomime the use of visually presented objects with form agnosia cannot perceive contours, although and have a superior naming of actions than of they can perceive brightness, color or luster. Associative visual agnosia results from left have a better recognition of moving than of static or bilateral occipito-temporal lesions. In contrast, patients with integrative agnosia the term optic aphasia is also found. It refers to a perceive single contours but cannot integrate them syndrome closely linked to visual agnosia and to in a coherent structure of the object, and produce transcortical sensory aphasia, and is often found predominantly visual similarity errors. Patients have a dispropor visual agnosia is due to bilateral occipital or occipito tionate difficulty in naming stimuli presented visually, temporal lesions.
Know that micropenis may result from hypopituitarism or primary defects in testosterone secretion or action 2 best antibiotics for sinus infection mayo clinic proven 200 mg doxycycline. Know the lower limit of normal phallic length at each stage of pubertal development 4 zinnat antibiotic cheap 100mg doxycycline fast delivery. Know the average chronologic and bone ages for spermarche and the relationship to early and late puberty c virus 1999 order line doxycycline. Know the age and Tanner stage-associated changes in ovarian and testicular steroid and pituitary hormone secretion b antibiotic induced fever generic 100 mg doxycycline amex. Know how to differentiate abnormal hormone changes from those of the normal "minipuberty" of male and female infants 3 antibiotic 48 hours order 100mg doxycycline fast delivery. Know the concentrations of sex steroids and gonadotropins in the newborn (full-term and preterm) and the changes in concentrations during the first days after birth b antimicrobial 7287 msds buy doxycycline 100mg on line. Know how midchildhood hormone levels during the juvenile pause compare to those of younger children 2. Know the hormonal determinants of the endometrial cycle and the changes in the endometrium that occur 3. Know the endocrine functions of the human placenta in terms of steroid and peptide production 2. Know the effects on the fetus of glucocorticoids administered to the pregnant woman 4. Recognize the causes of primary amenorrhea with sexual infantilism and primary amenorrhea with other signs of secondary sexual maturation. Know the similarities between amenorrhea induced by anorexia nervosa and by exercise 2. Know that defects causing hypogonadotropic hypogonadotropism are usually located in the anterior hypothalamus b. Recognize the patient with oophoritis/orchitis and the etiologies that may cause this g. Know that the central nervous system lesions associated with central precocious puberty are usually located in the posterior hypothalamus 4. Know that birth trauma and cerebral palsy are associated with central precocious puberty b. Recognize effects of precocious exposure to sex steroids on skeletal maturation 4. Distinguish familial gonadotropin-independent sexual precocity from central precocious puberty 3. Know the biochemical profile of a patient with an ovarian tumor and with an adrenal tumor 7. Know the differential diagnosis of hyperandrogenism in adolescent and adult females 9. Know the differential diagnosis of gynecomastia in prepubertal and pubertal boys 4. Recognize clinical disorders which result from excessive secretion of somatostatin b. Recognize that the metabolism of lipoproteins involves lipoprotein lipase, hepatic lipase, and lecithin-cholesterol acyl transferase 7. Know that patients with lipoprotein lipase deficiency present with hypertriglyceridemia, pancreatitis and xanthomas (eruptive) d. Know that the homozygous form of familial hypercholesterolemia is associated with coronary artery disease in the first two decades of life and high mortality f. Recognize that the phenotype of combined hyperlipidemia is associated with poorly controlled type 1 and type 2 diabetes g. Know that there is constitutive activation of adenylyl cyclase in McCune-Albright syndrome due to a somatic mutation in the stimulatory G protein. Know that Cushing syndrome may result from bilateral adrenocortical nodular hyperplasia in McCune-Albright syndrome 3. Know that Cushing syndrome may result from primary pigmented micronodular adrenocortical disease and know its association with Carney complex B. Be familiar with nonendocrine manifestations of autoimmune polyendocrine syndrome, type I 4. Understand the importance of family studies to determine linkage phase of mutations detected in an individual with a genetic disease 2. Understand the concept of a dominant negative mutation and the mechanisms involved b. Know the principles of methods used for determining binding capacity and affinity of receptors b. Understand that liganded cell-surface receptors often aggregate, are internalized into endosomes, and then can be recycled to the cell surface. Understand that intracellular receptors in the steroid hormone receptor superfamily bind to hormone response elements in promoters and alter transcription of target genes f. Recognize the potential effect of heterophilic/anti-animal antibodies on immunoassays and know that antibody effects may differ depending on whether the immunoassay is competitive or immunometric 2. Know that radioimmunoassays are based on competitive inhibition of the binding of labeled hormone to antibody by unlabeled hormone contained in standards and unknown samples and the methods involved 2. Recognize and understand the strengths and limitations of a cohort study, case control study, and randomized controlled clinical trial b. Assess how the data source (eg, diaries, billing data, discharge diagnostic code) may affect study results 3. Understand factors that affect the rationale for screening for a condition or disease (eg, prevalence, test accuracy, risk benefit, disease burden, presence of a presymptomatic state) 7. Understand the federal regulatory definition of minimal risk and apply this to research involving children. Particular focus has been placed on evidence-based models that might be utilized with under or uninsured populations seeking care among safety net providers. The following toolkit summarizes research fndings for primary care practices interested in pursuing this type of programming. Assistant Professor Director, Pediatric Obesity and Health Behavior Laboratory Pennington Biomedical Research Center Neelima Gonugunta, M. Research Trainee, Pediatric Obesity and Health Behavior Laboratory Pennington Biomedical Research Center Kathryn T. Assistant Professor Director, Contextual Risk Factors Laboratory Pennington Biomedical Research Center John C. Hodges Undergraduate Trainee, Pediatric Obesity and Health Behavior Laboratory Pennington Biomedical Research Center Timothy Nguyen Creative Media Specialist Pennington Biomedical Research Center Nhi Nguyen Graphic Designer Pennington Biomedical Research Center Table of Contents Clinical Assessment of Program Components Model Programs for 04 Childhood Obesity 14 that Enhance Efficacy 20 Childhood Obesity for Weight Loss Treatment Stages of Treatment for Special Considerations References 10 Childhood Obesity 18 for Underinsured 22 Populations Preventive Services Task Force recommends that clinicians screen children aged 6 years and older for obesity and offer them or refer them to comprehensive, intensive behavioral intervention to promote improvement in weight status. Centers for Disease Control and Prevention Growth Chart to account for sex and height differences in growth during childhood. Specifc family eating practices such as where the food is eaten and how the food is offered should also be assessed. Ask patient about any physical activity in the past week: Patient is obese if 95th percentile. Does patient do lifestyle activity like taking the 31 31 stairs instead of elevators, etc. He used to optimal range; elicit response; drink a lot of soda, but now I try to give him water whenever possible. Which of these, if either of them, do you think you and your child could interested in changing or which might be change My mother died of diabetes, and it wasnt pretty; maybe if he started showing signs of it; maybe if I could get into cooking a bit more. The major goal in the treatment of obese children and adolescents is for a child to develop healthy lifestyle habits that ultimately improve health and well-being in the long-term. In young obese children or mildly obese children, weight maintenance is the major focus rather than weight loss as they have not yet attained adult height. For further information, consult the Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity endorsed by the American Academy of Pediatrics3 and a recent overview of the prevention and treatment of pediatric obesity. Assist professional offers support and structure to a child to achieve the families in identifying current behaviors, cultural preferences, Stage 1 behaviors. Behavior change goals include: individual financial situations, daily schedules, and the safety of their neighborhood. These factors might be the barriers to adopting 1) Child and/or parent maintains a log to monitor the behaviors, healthy eating and physical activity habits. Work with the family to such as daily screen time and 3-day recording of food and determine target behaviors, such as: beverages consumed 2) Create a daily eating plan with structured daily meals and 1) Consume 5 servings of fruits and vegetables per day planned snacks (done by a registered dietitian or a physician ( The physician may refer the patient to Stage 1 can take place in the clinic setting. Depending on the needs of the individual child and family, visit frequency is based on the motivation of the patients and their a physician may offer a referral to an exercise therapist in order to families, or the severity of obesity. The following target behaviors and Food and Drug Administration for the treatment of childhood components should be integrated: obesity. Efficacy of this 7 1) A structured program with food monitoring, short-term diet and physical activity goal setting, and a contingency medication is modest only when used in conjunction with diet and management plan exercise. Typically sessions is required for children <12 years of age older a highly restrictive diet is the first step, followed by a mildly children may require less assistance from their parents restrictive diet, though there are no published data on long-term 4) Parents should learn how to modify the home environment outcomes for children. Primary care physicians should identify local resources like non-alcoholic steatosis) child psychologists and community resources. Weekly follow-up activities of daily living or quality of life, dyslipidemia, sleep visits for at least 8 to 12 weeks are useful to monitor and sustain new behaviors. Group visits may be more cost-effective and offer additional apnea with apnea-hypopnea index >15) benefits to the patient. Patients should be closely evaluated based on age, severity of obesity, motivation and emotional development, prior efforts to control weight, and family support before entering an intensive weight loss program. Providers reported increased self-effcacy to children and families at every offce visit. A typical primary care clinical setting model geared towards addressing acute conditions may not be structured to handle multidisciplinary management of chronic conditions like pediatric obesity where patient self-education plays a major role. Initially, the patient or the levels by controlling television watching and other screen time family is unaware of the problem. Once the parent recognizes and engaging their child in unstructured play or age-appropriate the problem, a clinician can motivate the person to work household chores. Also, group therapy lowers the provider to patient ratio thereby saving Various techniques of motivational interviewing are taught time and resources. This family-based approach can produce to pediatricians and registered dietitians in the primary care signifcant weight losses in both short and long term. Later, clinicians can teach more affordable and accessible for the general population and children and adolescents to enhance their general ability to self show potential as modes to deliver health and weight management regulate food intake using various behavioral change techniques. Accelerometers distinguish early time frame may how fast a person is moving to signifcantly improve determine the intensity level of the chances for physical activity a person has successful weight loss completed. These devices identifying children who have become more sophisticated do not successfully change in recent years. Commercially weight during the frst 3 available physical activity trackers months may help clinicians. Nike FuelBand, Fitbit, Jawbone) to explore alternative treatment have become more affordable and easier options rather than continuing an to wear, which may help clinicians, patients, ineffective behavioral program. Follow-up assessment is essential to ensure the long-term reduction in weight and long-term improvement in cardiovascular risk Other popular technologies can be used to promote physical factors. Follow-up assessment will also help to ensure that positive activity or healthy eating. For instance, mobile health technologies behavior changes like healthy dietary and physical activity habits including smartphone applications provide additional ways for are maintained once a child has completed the intensive program. A meta-analysis found 40 obesity treatment or prevention studies that included minority children. Parental involvement, culturally-based adaptation of program materials, and integrating interactive computer programs were all effective strategies for producing weight change in children. The health care team, child, and caregivers should mutually the primary care provider should routinely discuss obesity agree on treatment goals. Consider cultural, individual, and family preferences and the Efforts should prevent gestational diabetes mellitus and low realities of time and money in advice regarding meal planning. Consider cultural and gender preferences with regard to advice Health care providers should play an active role in advocacy about physical activity. This of low nutritional value evidence needs to be expanded through more studies targeting Promotion of regular physical activity and healthy food children of lower socioeconomic and income levels and non choices in schools white race/ethnicity. Provision of safe places for children to play and access to healthy food choices in underresourced neighborhoods Although some evidence suggests that the effects of weight loss medications or bariatric surgery may differ among racial or ethnic groups, decisions about the use of these interventions in children should not be based on race or ethnicity. Harvard Medical School Department of Population Medicine and Harvard Vanguard Medical Associates. The program has been implemented in a variety of are utilized to help families reach their goals. The program also settings for over 30 years and is continually reviewed and revised gives advice to families to help them reduce television viewing and to refect updated research and clinical applications regarding child consumption of sugary beverages and fast food. The program is designed for overweight children and is particularly sensitive to the needs of Mind, Exercise, Nutrition, minority youth living in an urban environment.
References
- Willett W. Nutritional Epidemiology. 3rd ed. New York: Oxford University Press; 2013.
- Brogan GX, Jr, Giarrusso E, Hollander JE, et al: Comparison of plain, warmed, and buffered lidocaine for anesthesia of traumatic wounds. Ann Emerg Med 26:121-125, 1995.
- Cals N, Devuyst G, Afsar N, et al. Pure superficial posterior cerebral artery territory infarction in The Lausanne Stroke Registry. J Neurol 2002;249(7):855-61.
- Burton CM, Iversen M, Scheike T, Carlsen J, Andersen CB. Is lymphocytic bronchiolitis a marker of acute rejection? An analysis of 2,697 transbronchial biopsies after lung transplantation. J Heart Lung Transplant 2008;27:1128-34.
- Aroner SA, Collins LC, Schnitt SJ, Connolly JL, Colditz GA, Tamimi RM. Columnar cell lesions and subsequent breast cancer risk: a nested case-control study. Breast Cancer Res. 2010;12(4):R61.
- Ji JS, Lee BI, Choi KY, et al. Diagnostic yield of tissue sampling using a bite-on-bite technique for incidental subepithelial lesions. Korean J Intern Med. 2009;24:101-105.
- Vaughan G, Grazie O, Graham D, et al. The use of pylric exclusion in the management of severe duodenal injuies. Am J Surg. 1977;134:785.
- Davis NB, Taber DA, Ansari RH, et al. Phase II trial of PS-341 in patients with renal cell cancer: A University of Chicago phase II consortium study. J Clin Oncol. 2004;22:115-119.