
Epitol
Rochelle Rubin, PharmD, BCPS, CDE
- Senior Clinical Pharmacy Coordinator�Family Medicine
- Assistant Residency Program Director�PGY1 Pharmacy Residency, The Brooklyn Hospital Center
- Clinical Assistant Professor of Pharmacy Practice, Arnold and Marie Schwartz College, Long Island University, Brooklyn, New York
However medications xl order generic epitol on line, no clear link with any specific neurobiological factors has been established treatment interstitial cystitis order online epitol. The disorder has not been identified in children who experience social neglect only after age 2 years symptoms pink eye buy epitol 100mg low price. Prognosis is only modestly associated with quality of the caregiving environment following serious neglect medicine hat mall cheap 100mg epitol with mastercard. In many cases medicine runny nose buy generic epitol on-line, the disorder persists treatment of diabetes order epitol master card, even in children whose caregiving environment becomes markedly improved. Comorbidity Limited research has examined the issue of disorders comorbid with disinhibited social engagement disorder. Exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways: 1. Learning that the traumatic event(s) occurred to a close family member or close friend. In cases of actual or threatened death of a family member or friend, the event(s) must have been violent or accidental. Experiencing repeated or extreme exposure to aversive details of the traumatic event(s). Note: Criterion A4 does not apply to exposure through electronic media, television, movies, or pictures, unless this exposure is work related. Note: In children older than 6 years, repetitive play may occur in which themes or aspects of the traumatic event(s) are expressed. Recurrent distressing dreams in which the content and/or affect of the dream are related to the traumatic event(s). Persistent avoidance of stimuli associated with the traumatic event(s), beginning after the traumatic event(s) occurred, as evidenced by one or both of the following: 1. Avoidance of or efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s). Negative alterations in cognitions and mood associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by two (or more) of the following: 1. Persistent and exaggerated negative beliefs or expectations about oneself, others, or the world. Persistent, distorted cognitions about the cause or consequences of the traumatic event(s) that lead the individual to blame himself/herself or others. Dereaiization: Persistent or recurrent experiences of unreality of surroundings. Specify if: With delayed expression: If the full diagnostic criteria are not met until at least 6 months after the event (although the onset and expression of some symptoms may be immediate). In children 6 years and younger, exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways: 1. Presence of one (or more) of the following intrusion symptoms associated with the traumatic event(s), beginning after the traumatic event(s) occurred: 1. Recurrent, involuntary, and intrusive distressing memories of the traumatic event(s). Note: It may not be possible to ascertain that the frightening content is related to the traumatic event. Intense or prolonged psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event(s). One (or more) of the following symptoms, representing either persistent avoidance of stimuli associated with the traumatic event(s) or negative alterations in cognitions and mood associated with the traumatic event(s), must be present, beginning after the event(s) or worsening after the event(s): Persistent Avoidance of Stimuli 1. Avoidance of or efforts to avoid activities, places, or physical reminders that arouse recollections of the traumatic event(s). Avoidance of or efforts to avoid people, conversations, or interpersonal situations that arouse recollections of the traumatic event(s). Alterations in arousal and reactivity associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by two (or more) of the following: 1. The disturbance causes clinically significant distress or impairment in relationships with parents, siblings, peers, or other caregivers or with school behavior. In some individuals, fear-based reexperiencing, emotional, and behavioral symptoms may predominate. In others, anhedonic or dysphoric mood states and negative cognitions may be most distressing. In some other individuals, arousal and reactive-externalizing symptoms are prominent, while in others, dissociative symptoms predominate. The directly experienced traumatic events in Criterion A include, but are not limited to , exposure to war as a combatant or civilian, threatened or actual physical assault. For children, sexually violent events may include developmentally inappropriate sexual experiences without physical violence or injury. The disorder may be especially severe or long-lasting when the stressor is interpersonal and intentional. Commonly, the individual has recurrent, involuntary, and intrusive recollections of the event (Criterion Bl). The emphasis is on recurrent memories of the event that usually include sensory, emotional, or physiological behavioral components. A common reexperiencing symptom is distressing dreams that replay the event itself or that are representative or thematically related to the major threats involved in the traumatic event (Criterion B2). Such events occur on a continuum from brief visual or other sensory intrusions about part of the traumatic event without loss of reality orientation, to complete loss of awareness of present surroundings. For young children, reenactment of events related to trauma may appear in play or in dissociative states. The individual commonly makes deliberate efforts to avoid thoughts, memories, feelings, or talking about the traumatic event. Negative alterations in cognitions or mood associated with the event begin or worsen after exposure to the event. These negative alterations can take various forms, including an inability to remember an important aspect of the traumatic event; such amnesia is typically due to dissociative amnesia and is not due to head injury, alcohol, or drugs (Criterion Dl). Problems with sleep onset and maintenance are common and may be associated with nightmares and safety concerns or with generalized elevated arousal that interferes with adequate sleep (Criterion E6). Associated Features Supporting Diagnosis Developmental regression, such as loss of language in young children, may occur. Lower estimates are seen in Europe and most Asian, African, and Latin American countries, clustering around 0. Highest rates (ranging from one-third to more than onehalf of those exposed) are found among survivors of rape, military combat and captivity, and ethnically or politically motivated internment and genocide. Symptoms usually begin within the first 3 months after the trauma, although there may be a delay of months, or even years, before criteria for the diagnosis are met. Duration of the symptoms also varies, with complete recovery within 3 months occurring in approximately one-half of adults, while some individuals remain symptomatic for longer than 12 months and sometimes for more than 50 years. Symptom recurrence and intensification may occur in response to reminders of the original trauma, ongoing life stressors, or newly experienced traumatic events. Young children may report new onset of frightening dreams without content specific to the traumatic event. Parents may report a wide range of emotional or behavioral changes in young children. Adolescents may harbor beliefs of being changed in ways that make them socially undesirable and estrange them from peers. Reckless behavior may lead to accidental injury to self or others, thrill-seeking, or high-risk behaviors. In older individuals, the disorder is associated with negative health perceptions, primary care utilization, and suicidal ideation. Risk and Prognostic Factors Risk (and protective) factors are generally divided into pretraumatic, peritraumatic, and posttraumatic factors. These include lower socioeconomic status; lower education; exposure to prior trauma (especially during childhood); childhood adversity. These include female gender and younger age at the time of trauma exposure (for adults). Finally, dissociation that occurs during the trauma and persists afterward is a risk factor. These include negative appraisals, inappropriate coping strategies, and development of acute stress disorder. The diagnosis requires that trauma exposure precede the onset or exacerbation of pertinent symptoms. Neither the arousal and dissociative symptoms of panic disorder nor the avoidance, irritability, and anxiety of generalized anxiety disorder are associated with a specific traumatic event. The symptoms of separation anxiety disorder are clearly related to separation from home or family, rather than to a traumatic event. Comorbid substance use disorder and conduct disorder are more common among males than among females. Exposure to actual or threatened death, serious injury, or sexual violation in one (or more) of the following ways: 1.
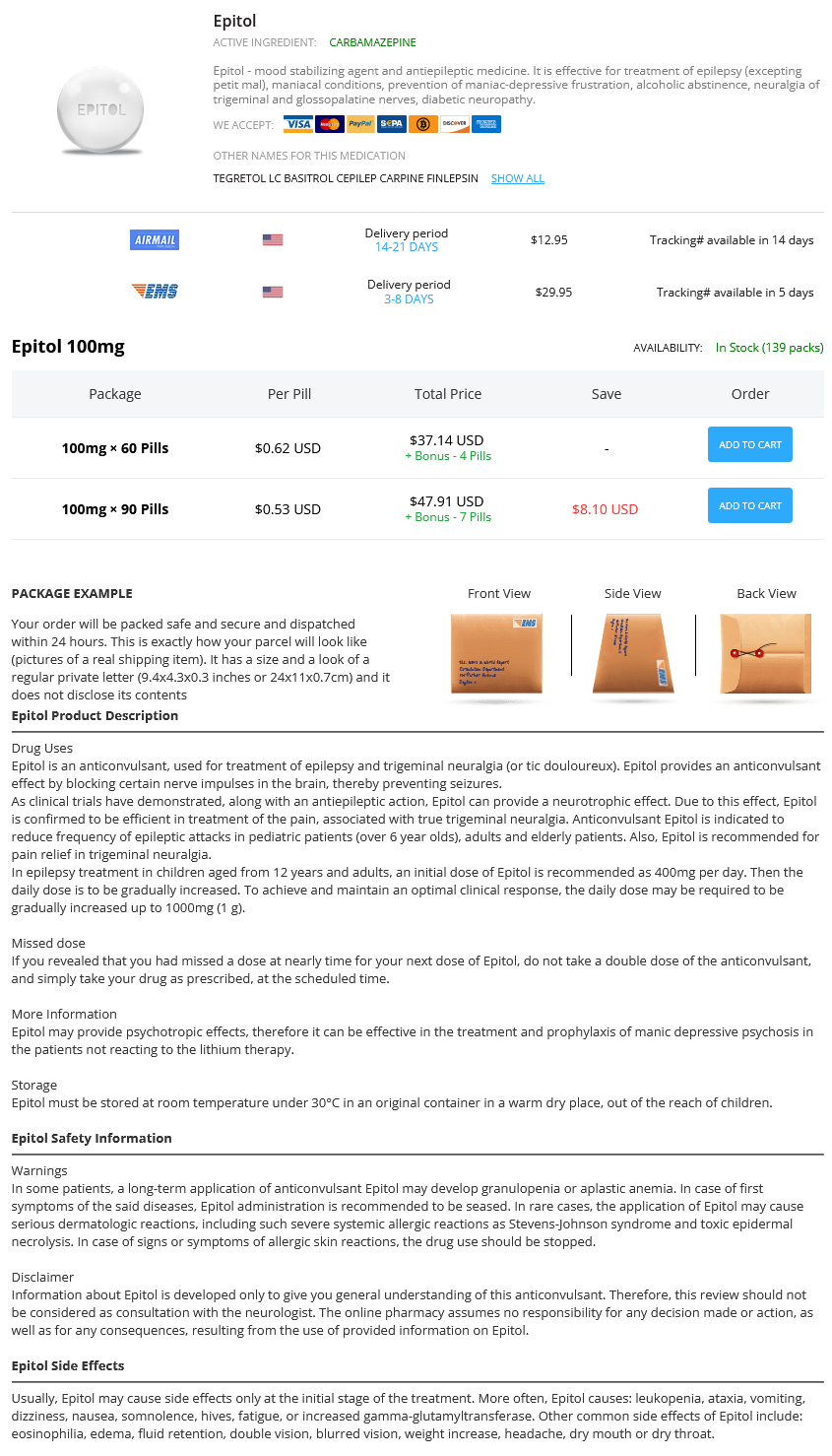
Some of these contain a preservative 5 medications for hypertension buy epitol 100 mg otc, to prevent contamination once the vial has been opened medications identification generic epitol 100 mg otc. Other substances treatment 5th metatarsal base fracture cheap epitol 100mg fast delivery, such as formaldehyde shakira medicine order epitol once a day, can be used during the production of vaccines acne natural treatment quality epitol 100 mg. All these substances are removed from the fnal product medicine cat herbs order genuine epitol line, but tiny traces of them, too small to have a clinical efect, can remain. For example: Mercury: Babies are exposed to mercury in milk, including breast milk. Formaldehyde: Formaldehyde is in automobile exhaust; in household products and furnishings such as carpets, upholstery, cosmetics, paint, and felt-tip markers; and in health products such as antihistamines, cough drops, and mouthwash. Aluminum: the average person takes in an estimated 30 to 50 mg of aluminum every day, mainly from foods, drinking water, and medicines. But if you search the web you can easily fnd a dozen websites that persist in claiming that they do. About 1% to 5% of the time, depending on the vaccine, a child who is vaccinated fails to develop immunity. For example, a single dose of measles vaccine protects about 95% of children, but after two doses almost 100% are immune. Sometimes a child gets sick with something that is similar to a disease they have been vaccinated against. Many viruses cause symptoms that look like fu, and people even call some of them fu, even though they are really not. With live vaccines, some children get what appears to be a mild case of disease (for example what looks like a measles or chickenpox rash but with only a few spots). One exception was the live oral polio vaccine, which could very rarely mutate and actually cause a case of polio. School immunization laws are not imposed by the federal government, but by the individual states. Remember that vaccines protect not only the person being vaccinated but also people around them. Immunization laws exist not only to protect individual children, but to protect all children. This would lead to levels of immunity dropping below what are needed for herd immunity (see page 37), which would lead in turn to outbreaks of disease. So mandatory vaccination, while it might not be a perfect solution, is at least a practical solution to a difcult problem. However, these laws are not so much to prevent drivers from harming themselves, which you could argue is their right, but to prevent them from harming others, which is not. All states allow medical exemptions, so children who cannot safely receive certain vaccines (like Riley. Most states also allow religious exemptions for children whose religion prohibits vaccination. Finally, some states allow philosophic exemptions for people who oppose vaccination on non-religious grounds. To protect themselves and others, unvaccinated students may be prohibited from attending classes if there is an outbreak of a vaccine-preventable disease at their school or in their community. You can go to a public clinic or health department rather than to a private physician. Vaccinations are generally cheaper there, and may be free except for an administration charge. From the day a baby is born, her immune system is busy dealing with the thousands of germs she is exposed to as part of daily life. Autism is usually diagnosed during the same age range when children are getting their routine shots. Naturally, if enough children develop autism during these ages, sometimes it will be noticed within a day or two after a vaccination visit. Part Four Frequently Asked Questions 49 Also, it is a very common logical error to assume that because one event directly follows another, it must have been caused by it. The diference is that the idea of a rooster causing the sun to rise is ridiculous, while the idea that vaccines can cause autism sort of makes sense. But that belief is based on the observation that it has always happened that way in the past. They advised that money that could be used to fund more studies on vaccines and autism would be better spent on areas of autism research more likely to be productive. How do you explain the increase in the number of children with autism, and the fact that the increase corresponded with an increase in the number of vaccinations children getfl The rise in the number of autism cases can be explained, at least in large part, by the fact that autism is being recognized and diagnosed much more often than it used to be, and that many conditions that used to go by other names are now being called autism, or autism spectrum disorder. The number of autism cases may actually be rising, but much of the apparent increase can be accounted for by the fact that we simply recognize it more often. As for the correspondence between the rise in autism and the increase in the number of vaccinations, remember. The theory that vaccines cause autism has been extensively tested, and has come up short. Part Four Frequently Asked Questions 51 Disease Caused by Spread by Chickenpox Varicella Zoster virus Air, direct contact Diphtheria Corynebacterium diphtheriae Air, direct contact bacteria Hib Disease Haemophilus infuenzae type b Air, direct contact bacteria Hepatitis A Hepatitis A virus Personal contact. Sore throat, mild fever, membrane Heart failure, paralysis, pneumonia, in throat, swollen neck death. May be no symptoms unless bacteria Meningitis, epiglotittis, pneumonia, enter blood. Fever, headache, malaise, vomiting, Chronic infection, cirrhosis, liver failure, arthritis. Swollen salivary glands, fever, headache, Meningitis, encephalitis, infammation malaise, muscle pain. Diarrhea, fever, vomiting Severe diarrhea, dehydration, electrolyte imbalance, kidney and liver disease, death Rash, fever, lymphadenopathy, malaise. Stifness in neck, difculty swallowBroken bones, breathing difculty, ing, rigid abdominal muscles, muscle death. With vaccines, a local reaction usually refers to redness, soreness or swelling where an injection was given. A reaction that afects the body as a whole, such as a fever or bacteremia, is called a systemic reaction. Paralysis usually occurs in the arms or legs, but any muscle can become paralyzed, including those that control breathing. A seizure can have many causes, including epilepsy or other brain disorders, or a high fever (see febrile seizure). Someone who has never had a disease or been vaccinated against it is susceptible to that disease. Includes chapters about foreign travel, how vaccines work and how they are made, and safety. Another good introduction, which answers many of the questions parents have about childhood vaccinations. Written for healthcare providers, it also contains information of interest to parents. Available online, or may be purchased through the Public Health Foundation (see Internet You can fnd vast amounts of information about vaccinations on the internet. The problem is that, unlike with book publishing, there are few controls on internet materials. Anyone can create a website or blog and say anything they want to say without having to back it up. Of course there is no sure way to know whether information on a website is accurate or not, but several websites ofer suggestions for evaluating web content. Acknowledgments the following are thanked for submitting their drawings for use in this publication: Adriana Toungette, Alejandro Macias, Alex Cordon, Amber Blakely, Andwon Tyson, Brandon Rosillo, Cynthia Reys, Daniel Orta, Dioner Gala, Estefany, Evn Marilyn Benson, Gihasel Kahn, Henock, Iyana Williams, Jocelyn Kopfman, Jonathan Moore, Kyle Smith, Maggie Desantos, Manuela Rahimic, Marisol Baughman, Melissa Lopez, Moises, Nataly Leal, Nataneal Nistor, Ramon Perez, Riley Wright, Sam Toungette, Trent L. The economic impact of epilepsy represents estimated direct and indirect costs of 12. Patients with this disorder experience increased morbidity and mortality with long term fatality rates of 24%. In these intractable epilepsy patients, non-pharmacological treatments can be considered. Commonly used non-pharmacological treatment options for epilepsy include epilepsy surgery, neurostimulation therapy, and diet therapy. Keywords: Epilepsy; Seizure epilepsy patients married or had children, higher education or achievement in later life than the general population [4,5,10,14,15]. Introduction Also, patients with poorly controlled epilepsy experience decline in memory and cognition [10,12,14,15,17]. Co-morbid mood disorders A seizure is a clinical manifestation, resulting from a brief episode such as depression and anxiety are common and more prevalent in of abnormal excessive or synchronous neuronal activity in the brain. Epilepsy is a braindisorder characterized by a chronic predisposition In these uncontrolled patients, other treatment options are available to generate epileptic seizures with secondary neurobiologic, cognitive, and dependentupon the seizure type, localization of seizure onset, age, psychological, and social consequences.
It again has limited drug-drug interaction medications not to take when pregnant order epitol 100mg with amex, has no significant adverse effect on cognition Carbamazepine medicine rash generic epitol 100 mg otc, an enzyme inducer medications elavil side effects purchase epitol 100 mg on line, is a possible symptoms night sweats buy epitol 100 mg with mastercard, but not preferred symptoms indigestion buy 100mg epitol fast delivery, option in the treatment of epilepsy in and is generally well tolerated medications definition purchase 100 mg epitol. Sedative effects may limit tolerability but can be minimised by starting with a very low dose and slow upward titration. Intra-dosage variation Overall, the current treatment choice for chronic treatment of older people with epilepsy probably rests in concentrations of carbamazepine, which are related to the extent of autoinduction of metabolism25-26, with low-dose monotherapy with Lamotrigine or Levetiracetam. Once or twice-daily dosing with conventional carbamazepine valproate and possibly Carbamazepine are alternatives. While the overall risk of bone marrow suppression and hepatitis is small less favoured owing to potential impact on cognition and other side effects. Carbamazepine has an antidiuretic hormone-like effect, and this very novel anti-epileptic medications, for example Perampanel or Brivaracetam, in the elderly. Carbamazepine may precipitate problems with cardiac conduction in Whichever drug is used the introductory dose should be low and dose titration should be slow and cautious. There are also concerns about its potential effects on bone Monitoring for potential side effects should be intensive and due consideration should be given to the health. Therapeutic but there is no definitive data regarding its use in this age group and there are concerns particularly with ranges are less helpful in elderly people. National General Practice Study of Epilepsy: newly diagnosed epileptic seizures in a general population. Predictors of incident epilepsy in older adults: the Older patients with pharmacoresistant epilepsy are less likely to undergo epilepsy surgery which may Cardiovascular Health Study. Clinically unsuspected cerebral infarction revealed by computed over 75 years of age. However, as the population ages distinctions will be made between biological and tomography scanning in late onset epilepsy. Epilepsy surgery in older patients can associate with reduced likelihood of seizure freedom and increased Cogn. Value of clinical features, electroencephalography, and than 50, seizure freedom rates at one year were reported to be similar34. However, the rate of post-operative computerised tomographic scanning in prediction of seizure recurrence. Seizure recurrence after a 1st unprovoked seizure: an extended cognitive impairment was substantially higher in older individuals, particularly those undergoing left follow-up. Furthermore, older patients undergoing epilepsy surgery had lower pre-operative 16. Multicentre comparative trial of sodium valproate and phenytoin in elderly patients with newly in individuals with poor reserve could precipitate significant difficulties in daily life. Impact of valproate and phenytoin on cognitive function in elderly patients: results of a single-blind randomized comparative study. Cognitive effects of anticonvulsant monotherapy in elderly patients: a placeboutilising the same operative technique, no difference in post-operative outcome in terms of either seizure controlled study. Multicentre, double-blind, randomised comparison between lamotrigine and carbamazepine in elderly patients with newly diagnosed epilepsy. Intradose and circadian variation in circulating carbamazepine and its epoxide in epileptic patients: a consequence of autoinduction of metabolism. The effects of age on carbamazepine pharmacokinetics with psychosocial difficulties. Often an underlying illness (stroke, dementia) is responsible for the development of seizures and older 26. Moreover, depression, which may increase cognitive difficulties, can be compounded by 28. Epilepsy Surgery: Factors That Affect Patient DecisionMaking in Choosing or Deferring a Procedure. Outcome of temporal Epilepsy is already very common in the older population and the incidence will rise as populations age. Diagnosis can be difficult but, as for all epilepsy, rests on securing a detailed history. Outcomes after resective epilepsy surgery in patients over 50 years non-contributory and occasionally confusing. Seizure 2014; 23: 64 in this age group and in those with pharmacoresistant seizures, surgery can be considered. Surgery for temporal lobe epilepsy associated with mesial temporal sclerosis in the older patient: A long-term follow-up. A survey of epileptic disorders in southwest France: seizures in elderly patients. Sodium valproate can also stimulate appetite leading to obesity, as can vigabatrin, gabapentin and pregabalin. The occurrence of these side effects, which are mostly undesirable in all, can have a particularly detrimental effect during adolescence. Female hormones may also affect seizure threshold, resulting in increased frequency of seizures at certain times of the menstrual cycle. Hormonal alterations, including changes in prolactin, follicle-stimulating hormone and luteinising hormone have been observed following generalised and focal seizures1. Many of the problems An increase in seizure frequency around the time of menstruation (catamenial epilepsy) was frst clinically of tolerance, in particular those of benzodiazepines, can be overcome using this treatment model. In documented by Gowers in 1881 but cyclical variations in seizure frequency have been known about since a double-blind crossover study of 20 mg clobazam versus placebo over a predetermined ten-day period in antiquity and were initially attributed to the cycles of the moon. There is no agreement on the degree of seizure exacerbation required to meet a defnition of catamenial epilepsy. However, many of these With regard to therapy it should frst be established whether the seizures are truly catamenial, and the studies are poorly documented, use a less than strict defnition of what seizures to include in the calculation particular subtype of catamenial epilepsy, and that the menses are following a regular pattern23. If so, of perimenstrual attacks and are unrepresentative of the female population with epilepsy. Using the strict intermittent therapy with clobazam 10 mg at night perimenstrually is the simplest and most useful defnition for catamenial epilepsy that fl 75% of seizures have to occur within four days preceding and therapy for the majority of women. If this fails, it may be worth considering the use of acetazolamide within six days of the onset of menstruation, Duncan et al showed that only 12. However, 31 (78%) claimed that most of their seizures occurred around the time of menstruation. However, good evidence for the effectiveness of these therapeutic options is lacking. Human data tend to support this hypothesis, although there appear to be no clear Fertility differences in hormonal changes in women with and without catamenial seizures7. The potential reasons for this are allopregnanolone withdrawal at the time of menstruation (day 25 of the outgoing cycle to day 3 of new likely to be complex, and include social and economic factors. It has also been reported that sexual cycle) provide one possible mechanism for exacerbation of seizures perimenstrually (which is the most arousal may be reduced in women with epilepsy. However the situation is far from resolved, with other common type of catamenial seizure exacerbation), although other mechanisms have also been suggested8. The second most common pattern observed is the periovulatory pattern, where increased seizure frequency It is recognised that there is a high incidence of menstrual disorders among women with epilepsy26. Anovulatory cycles tend to be 35% of women with partial seizures of temporal lobe origin had anovulatory cycles when studied over associated with higher seizure frequencies, in particular during times of peak oestrogen concentration10. Treatment has been tried with progesterone suppositories Anovulatory cycles tend to be associated with an increase in seizure frequency in the second half of the in the appropriate phase of the menstrual cycle 28, as well as clomiphene24, and medroxyprogesterone17, menstrual cycle while ovulatory cycles can have one or two peaks in seizure frequency, at around the time with some success. A recent prospective study showed that women with epilepsy have an increased risk of infertility, Other infuences around the time of menstruation, such as premenstrual tension and mood changes, may particularly if they are using polytherapy. In 1993, Isojarvi reported that polycystic ovaries and Over the last century many therapeutic agents have been tried with various degrees of success. Subsequently they reported that these introduced bromides in 1857 for the treatment of catamenial and hysterical epilepsies. By the turn abnormalities are more common in women on valproate who gain weight31, especially if this is during of the century it had been noted that seizure frequency occasionally decreased at the menopause or pubertal maturation32. However, their initial study was retrospectively based in a selected population and after oopherectomy. In the 1950s acetazolamide became available, which is advocated by some for use did not concentrate on clinical endocrine status. Betts is based, however are scant, with no randomised controlled trials and conficting views on its effectiveness13,14. Over the last decade or so one of the main areas of therapeutic research has been hormonal manipulation. Topiramate is a less potent inducer of menstrual cycles were randomised to treatment with valproate or lamotrigine and followed up for hepatic enzymes, and this effect seems to be dose dependent. These observations, together with data showing that 35 micrograms of ethinyloestradiol. Bidirectional interactions can occur with seen at the lower doses of 4mg or 8mg53. If breakthrough bleeding occurs ethinyloestradiol dosages may need to be compared with the withdrawal method, barrier contraceptives, and hormonal contraception. Breakthrough bleeding occurring in the middle of a cycle of contraceptive use is generally due demonstrated a greater increase in seizures with the use of hormonal contraception (18%) compared with to a relative oestrogen defciency and usually taken as a sign of incipient failure of contraception48. However, pregnancy rates (approximately 7% per year) still appear to be lower compared with barrier methods which have a failure rate of between 15 and 20%. Medroxyprogesterone injections may be effective in women with epilepsy, with their and increased seizures in 9%45. Whether the dose of the morning-after pill should be changed in those on enzymeHaving epilepsy should not restrict the use of contraception. Oxcarbazepine is also contraceptive pill affecting levetiracetam lacosamide, or zonisamide metabolism. For example, for autosomal dominant conditions such as tuberous sclerosis there is a 1:2 risk of a child inheriting the the management of pregnant women with epilepsy is becoming of increasing importance as the risk factors condition. The increasing evidence base recessive and there is therefore a low risk of children developing the condition. The risk of a child for management has also resulted in expert and national groups forming guidelines to aid management, developing epilepsy is dependent on the type of seizure disorder and the number of affected relatives. For the majority of women with epilepsy will have a normal pregnancy and delivery, an unchanged seizure primary generalised seizure disorders there is up to a 10% chance of offspring developing epilepsy but frequency and over a 90% chance of a healthy baby. Because of this, pregnancies in women with to be lower if only the father has epilepsy compared with if only the mother has epilepsy66. Folic acid Preconception Theprescriptionoffolicacidbeforeconceptionandatleastuntiltheendofthefrsttrimesterisrecommended Preconception counselling should be available to all women with epilepsy contemplating a pregnancy. This followed the recognition that there this should start at the time of diagnosis and at subsequent reviews. Large community-based studies have demonstrated a reduction in the be considered in female adolescents with epilepsy, including those whose care is being transferred from rate of neural tube defects in women taking folic acid pre-conceptually 70, 71,72. The fact that the relevant issues have been discussed should always this that folic acid will protect women with epilepsy who are also at increased risk of this complication. Women with epilepsy of childbearing years do not always recall being the optimum dosage of folic acid remains undetermined. Community-based studies have used dosages given relevant information, hence the need to repeat this regularly. Ideally an organised joint obstetric/neurology pre-conceptual counselling service should be available Some concerns have been raised that folic acid may exacerbate seizures but these fears have generally to allow rapid assessment of women actively contemplating pregnancy and to coordinate care during been felt to be unfounded. There is as yet no direct evidence that folic acid will protect against the neural pregnancy63. There is some evidence that the in epilepsy, this is not always available and waiting times are long. Nevertheless, a re-confguration neural tube defects, which occur in association with sodium valproate, are somewhat different from those of clinics and additional resources to allow for this service should be actively considered. Other abnormalities are less common and the defect may be the result of altered canalisation rather than folding of the developing During counselling a re-evaluation of the diagnosis and the need for continued antiepileptic medication neural crest. It remains uncertain as to whether folic acid will protect against this form of neural tube should take place. Details likely to have a child with a major congenital malformation than those who did not (3.
The appearance preoccupation is not better explained by concerns with body fat or weight in an individual whose symptoms meet diagnostic criteria for an eating disorder medicine 3604 generic epitol 100mg otc. Specify if: With muscle dysmorphia: the individual is preoccupied with the idea that his or her body build is too small or insufficiently muscular treatment 1st degree heart block discount 100 mg epitol. With poor insight: the individual thinks that the body dysmorphic disorder beliefs are probably true treatment knee pain generic epitol 100 mg free shipping. With absent insight/delusionai beliefs: the individual is completely convinced that the body dysmorphic disorder beliefs are true medicine 7 year program purchase genuine epitol. The perceived flaws are not observable or appear only slight to other individuals medicine 4h2 pill effective 100mg epitol. Concerns range from looking "unattractive" or "not right" to looking "hideous" or "like a monster medicine 0025-7974 100 mg epitol free shipping. The preoccupations are intrusive, unwanted, time-consuming (occurring, on average, 3-8 hours per day), and usually difficult to resist or control. Compulsive skin picking intended to improve perceived skin defects is common and can cause skin damage, infections, or ruptured blood vessels. A majority (but not all) diet, exercise, and/or lift weights excessively, sometimes causing bodily damage. Insight regarding body dysmorphic disorder beliefs can range from good to absent/ delusional. On average, insight is poor; onethird or more of individuals currently have delusional body dysmorphic disorder beliefs. Individuals with delusional body dysmorphic disorder tend to have greater morbidity in some areas. Associated Features Supporting Diagnosis Many individuals with body dysmorphic disorder have ideas or delusions of reference, believing that other people take special notice of them or mock them because of how they look. Many individuals are ashamed of their appearance and their excessive focus on how they look, and are reluctant to reveal their concerns to others. Body dysmorphic disorder appears to respond poorly to such treatments and sometimes becomes worse. Some individuals take legal action or are violent toward the clinician because they are dissatisfied with the cosmetic outcome. Deveiopment and Course the mean age at disorder onset is 16-17 years, the median age at onset is 15 years, and the most common age at onset is 12-13 years. Subclinical body dysmorphic disorder symptoms begin, on average, at age 12 or 13 years. Subclinical concerns usually evolve gradually to the full disorder, although some individuals experience abrupt onset of body dysmorphic disorder. The disorder appears to usually be chronic, although improvement is likely when evidence-based treatment is received. Body dysmoflhic disorder occurs in the elderly, but little is known about the disorder in this age group. Individuals with disorder onset before age 18 years are more likely to attempt suicide, have more comorbidity, and have gradual (rather than acute) disorder onset than those with adult-onset body dysmorphic disorder. Culture-Reiated Diagnostic issues Body dysmorphic disorder has been reported internationally. It appears that the disorder may have more similarities than differences across races and cultures but that cultural values and preferences may influence symptom content to some degree. A substantial proportion of individuals attribute suicidal ideation or suicide attempts primarily to their appearance concerns. Functionai Consequences of Body Dysmorphic Disorder Nearly all individuals with body dysmorphic disorder experience impaired psychosocial functioning because of their appearance concerns. More severe body dysmorphic disorder symptoms are associated with poorer functioning and quality of life. Individuals may be housebound because of their body dysmorphic disorder symptoms, sometimes for years. D ifferential Diagnosis Normal appearance concerns and clearly noticeable physical defects. In an individual with an eating disorder, concerns about being fat are considered a symptom of the eating disorder rather than body dysmorphic disorder. Eating disorders and body dysmorphic disorder can be comorbid, in which case both should be diagnosed. These disorders have other differences, such as poorer insight in body dysmoflhic disorder. When hair removal (plucking, pulling, or other types of removal) is intended to improve perceived defects in the appearance of facial or body hair, body dysmoflhic disorder is diagnosed rather than trichotillomania (hairpulling disorder). However, major depressive disorder and depressive symptoms are common in individuals with body dysmoflhic disorder, often appearing to be secondary to the distress and impairment that body dysmorphic disorder causes. Body dysmoflhic disorder should be diagnosed in depressed individuals if diagnostic criteria for body dysmoflhic disorder are met. Unlike generalized anxiety disorder, anxiety and worry in body dysmoflhic disorder focus on perceived appearance flaws. Koro, a culturally related disorder that usually occurs in epidemics in Southeastern Asia, consists of a fear that the penis (labia, nipples, or breasts in females) is shrinking or retracting and will disappear into the abdomen, often accompanied by a belief that death will result. It involves symptoms reflecting an overconcern with slight or imagined flaws in appearance. Persistent difficulty discarding or parting with possessions, regardless of their actual value. This difficulty is due to a perceived need to save the items and to distress associated with discarding them. The difficulty discarding possessions results in the accumulation of possessions that congest and clutter active living areas and substantially compromises their intended use. If living areas are uncluttered, it is only because of the interventions of third parties. The hoarding is not better explained by the symptoms of another mental disorder. Specify if: With good or fair insight: the individual recognizes that hoarding-related beliefs and behaviors (pertaining to difficulty discarding items, clutter, or excessive acquisition) are problematic. With absent insight/deiusionai beliefs: the individual is completely convinced that hoarding-related beliefs and behaviors (pertaining to difficulty discarding items, clutter, or excessive acquisition) are not problematic despite evidence to the contrary. Approximately 80%-90% of individuals with hoarding disorder display excessive acquisition. The most frequent form of acquisition is excessive buying, followed by acquisition of free items. Individuals with hoarding disorder typically experience distress if they are unable to or are prevented from acquiring items. Diagnostic Features the essential feature of hoarding disorder is persistent difficulties discarding or parting with possessions, regardless of their actual value (Criterion A). The difficulty in discarding possessions noted in Criterion A refers to any form of discarding, including throwing away, selling, giving away, or recycling. The main reasons given for these difficulties are the perceived utility or aesthetic value of the items or strong sentimental attachment to the possessions. Some individuals feel responsible for the fate of their possessions and often go to great lengths to avoid being wasteful. The most commonly saved items are newspapers, magazines, old clothing, bags, books, mail, and paperwork, but virtually any item can be saved. This criterion emphasizes that the saving of possessions is intentional, which discriminates hoarding disorder from other forms of psychopathology that are characterized by the passive accumulation of items or the absence of distress when possessions are removed. For example, the individual may not be able to cook in the kitchen, sleep in his or her bed, or sit in a chair. Clutter is defined as a large group of usually unrelated or marginally related objects piled together in a disorganized fashion in spaces designed for other purposes. In some cases, living areas may be uncluttered because of the intervention of third parties. Individuals who have been forced to clear their homes still have a symptom picture that meets criteria for hoarding disorder because the lack of clutter is due to a third-party intervention. Hov^ever, any attempts to discard or clear the possessions by third parties result in high levels of distress. Associated Features Supporting Diagnosis Other common features of hoarding disorder include indecisiveness, perfectionism, avoidance, procrastination, difficulty planning and organizing tasks, and distractibility.
With poor insight: the individual thinks obsessive-compulsive disorder beliefs are probably true medications and mothers milk 2016 discount 100 mg epitol fast delivery. With absent insight/deiusionai beiiefs: the individual is completely convinced that obsessive-compulsive disorder beliefs are true medications medicaid covers purchase 100mg epitol otc. Specify if: Tic-reiated: the individual has a current or past history of a tic disorder treatment jellyfish sting buy 100mg epitol with amex. Importantly symptoms 3 days past ovulation generic epitol 100mg, obsessions are not pleasurable or experienced as voluntary: they are intrusive and unwanted and cause marked distress or anxiety in most individuals symptoms 9 dpo buy generic epitol on-line. Compulsions are not done for pleasure medicine while pregnant purchase epitol 100 mg overnight delivery, although some individuals experience relief from anxiety or distress. This criterion helps to distinguish the disorder from the occasional intmsive thoughts or repetitive behaviors that are common in the general population. Associated Features Supporting Diagnosis the specific content of obsessions and compulsions varies between individuals. However, certain themes, or dimensions, are common, including those of cleaning (contamination obsessions and cleaning compulsions); symmetry (symmetry obsessions and repeating. Some individuals also have difficulties discarding and accumulate (hoard) objects as a consequence of typical obsessions and compulsions, such as fears of harming others. While performing compulsions, some individuals report a distressing sense of "incompleteness" or uneasiness until things look, feel, or sound "just right. Females are affected at a shghtly higher rate than males in adulthood, although males are more commonly affected in childhood. Males have an earlier age at onset than females: nearly 25% of males have onset before age 10 years. The onset of symptoms is typically gradual; however, acute onset has also been reported. Some individuals have an episodic course, and a minority have a deteriorating course. The pattern of symptoms in adults can be stable over time, but it is more variable in children. Some differences in the content of obsessions and compulsions have been reported when children and adolescent samples have been compared with adult samples. Greater internalizing symptoms, higher negative emotionality, and behavioral inhibition in childhood are possible temperamental risk factors. Dysfunction in the orbitofrontal cortex, anterior cingulate cortex, and striatum have been most strongly implicated. Moreover, around the globe, there is a similar symptom structure involving cleaning, symmetry, hoarding, taboo thoughts, or fear of harm. However, regional variation in symptom expression exists, and cultural factors may shape the content of obsessions and compulsions. Avoidance of situations that can trigger obsessions or compulsions can also severely restrict functioning. For example, obsessions about harm can make relationships with family and friends feel hazardous; the result can be avoidance of these relationships. Obsessions about symmetry can derail the timely completion of school or work projects because the project never feels "just right," potentially resulting in school failure or job loss. When the disorder starts in childhood or adolescence, individuals may experience developmental difficulties. The result can be few significant relationships outside the family and a lack of autonomy and financial independence from their family of origin. Recurrent thoughts, avoidant behaviors, and repetitive requests for reassurance can also occur in anxiety disorders. However, the recurrent thoughts that are present in generalized anxiety disorder. In body dysmorphic disorder, the obsessions and compulsions are limited to concerns about physical appearance; and in trichotillomania (hair-pulling disorder), the compulsive behavior is limited to hair pulling in the absence of obsessions. A tic is a sudden, rapid, recurrent, nonrhythmic motor movement or vocalization. Tics and stereotyped movements are typically less complex than compulsions and are not aimed at neutralizing obsessions. However, they have obsessions and compulsions (distinguishing their condition from delusional disorder) and do not have other features of schizophrenia or schizoaffective disorder. Many adults with the disorder have a lifetime diagnosis of an anxiety disorder (76%;. Preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others. At some point during the course of the disorder, the individual has performed repetitive behaviors. Prevalence Nationally representative prevalence studies of hoarding disorder are not available. Hoarding disorder affects both males and females, but some epidemiological studies have reported a significantly greater prevalence among males. Hoarding symptoms appear to be almost three times more prevalent in older adults (ages 55-94 years) compared with younger adults (ages 34-44 years). Development and Course Hoarding appears to begin early in life and spans well into the late stages. Because children and adolescents typically do not control their living environment and discarding behaviors, the possible intervention of third parties. Individuals with hoarding disorder often retrospectively report stressful and traumatic life events preceding the onset of the disorder or causing an exacerbation. C ulture-Related Diagnostic issues While most of the research has been done in Western, industrialized countries and urban communities, the available data from non-Western and developing countries suggest that hoarding is a universal phenomenon with consistent clinical features. Appliances may be broken, and utilities such as water and electricity may be disconnected, as access for repair work may be difficult. In severe cases, hoarding can put individuals at risk for fire, falling (especially elderly individuals), poor sanitation, and other health risks. In these individuals, the hoarding behavior is not present prior to the onset of the brain damage and appears shortly after the brain damage occurs. Some of these individuals appear to have little interest in the accumulated items and are able to discard them easily or do not care if others discard them, whereas others appear to be very reluctant to discard anything. Hoarding disorder is not diagnosed if the accumulation of objects is judged to be a direct consequence of psychomotor retardation, fatigue, or loss of energy during a major depressive episode. The most common comorbid conditions are major depressive disorder (up to 50% of cases), social anxiety disorder (social phobia), and generalized anxiety disorder. The hair pulling or hair loss is not attributable to another medical condition. The hair pulling is not better explained by the symptoms of another mental disorder. Hair pulling may occur from any region of the body in which hair grows; the most common sites are the scalp, eyebrows, and eyelids, while less common sites are axillary, facial, pubic, and peri-rectal regions. Hair pulling may occur in brief episodes scattered throughout the day or during less frequent but more sustained periods that can continue for hours, and such hair pulling may endure for months or years. Criterion A requires that hair pulling lead to hair loss, although individuals with this disorder may pull hair in a widely distributed pattern. Associated Features Supporting Diagnosis Hair pulling may be accompanied by a range of behaviors or rituals involving hair. Hair pulling may also be preceded or accompanied by various emotional states; it may be triggered by feelings of anxiety or boredom, may be preceded by an increasing sense of tension (either immediately before pulling out the hair or when attempting to resist the urge to pull), or may lead to gratification, pleasure, or a sense of relief when the hair is pulled out. Some individuals experience an "itch-like" or tingling sensation in the scalp that is alleviated by the act of pulling hair. When the scalp is involved, there may be a predilection for pulling out hair in the crown or parietal regions.
Best 100mg epitol. depression tension / tension depression symptoms / can depression cause physical symptoms /.
References
- Cooper DJ. Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. Ann Intern Med. 1990;112(7):492.
- Feldman DR, Bosl GJ, Sheinfeld J, et al: Medical treatment of advanced testicular cancer, J Am Med Assoc 299:672n684, 2008.
- Hope P, Breslin S, Lamont L et al. Fatal shoulder dystocia: a review of 56 cases reported to the Confidential Enquiry into Stillbirths and Deaths in Infancy. Br J Obstet Gynaecol 1998; 105: 1256-61.
- Hirayama F, Lee AH, Binns CW, et al: Association of impaired respiratory function with urinary incontinence, Respirology 14:753n756, 2009.