
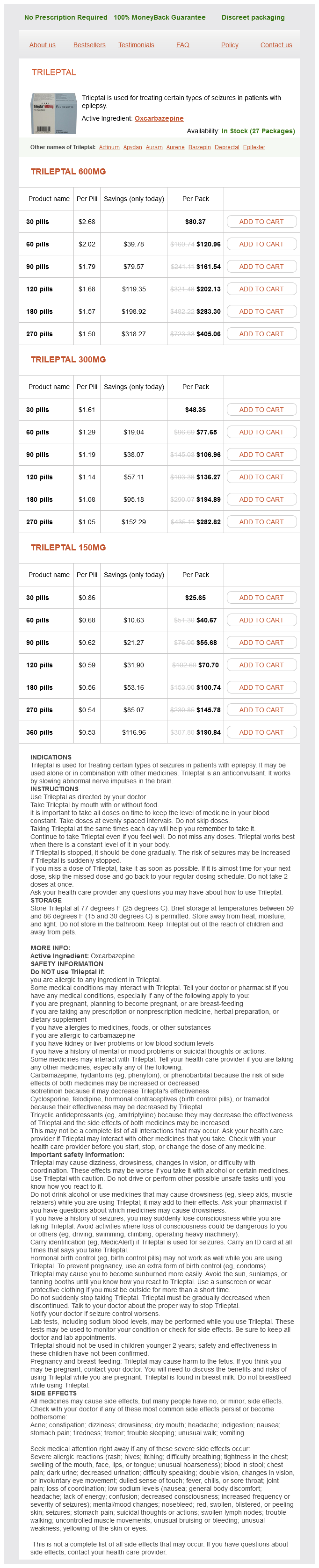
Trileptal
Vincent Lucente MD, MBA
- Clinical Professor of Obstetrics and Gynecology
- Division of Gynecology
- Department of Obstetrics and Gynecology
- Temple University College of Medicine
- Philadelphia, Pennsylvania
- Chief of Gynecology
- Division of Urogynecology
- Department of Obstetrics and Gynecology
- St. Luke? Hosptial
- Allentown, Pennsylvania
American Academy of Pediatrics Committee on Fetus and Newborn; American Academy of Pediatrics Section on Surgery; Canadian Paediatric Society Fetus and Newborn Committee medications requiring aims testing cheap trileptal 600 mg without a prescription. The American Academy of Pediatrics Committee on Environmental Health; Committee on Native American Child Health; Committee on Adolescence premonitory symptoms cheap trileptal 600mg free shipping. Committee on Quality Improvement medications covered by blue cross blue shield buy trileptal discount, Subcommittee on Developmental Dysplasia of the Hip treatment depression order trileptal 150mg online. International Consensus Conference on Intersex organized by the Lawson Wilkins Pediatric Endo crine Society and the European Society for Paediatric Endocrinology. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. American Academy of Pediatrics Section on Breastfeeding; American Academy of Pediatrics Committee on Nutrition. Neonatal Complications Anemia Anemia of prematurity results from multiple factors and varies with the degree of immaturity, illness, postnatal age, and nutrition. As growth accelerates with advancing postnatal age, depletion of iron stores begins to affect erythropoiesis. A multipronged approach to decreasing red blood cell transfusion is recom mended, particularly in very low birth weight infants, to address both causa tion and correction of anemia of prematurity. Two studies have suggested that restrictive transfusion guidelines could be associated with adverse neurodevelopmental effects. Thus, routine use of human recombinant erythropoietin in preterm infants is not supported by current evidence. Neurologic immaturity of respira tory control is hypothesized to be a common underlying mechanism. Persistent apnea often is associated with inadequate oral feeding, which may be the only remaining issue to be resolved before discharge from the hospital. Home cardiorespi ratory monitors are rarely indicated for detection of apnea solely because of immature respiratory control and should not be used to justify discharge of infants who are still at risk of apnea. Home cardiorespiratory monitoring may be useful for some infants who are technology dependent (see also Hospital Discharge of High-Risk Infants later in this chapter). Neonatal Complications and Management of High-Risk Infants 323 Brain Injury Hemorrhagic and Periventricular White Matter Brain Injury Infants born at 32 weeks of gestation or less or who have birth weights of 1,500 g or less are at highest risk of hemorrhagic and other brain injuries. Residual lesions after brain injury include minimal to extensive cystic lesions in the periventricular white matter and ventriculomegaly secondary to diffuse cerebral atrophy. These lesions evolve over the course of several weeks after the precipitating insult. Follow-up studies to monitor for the evolution of severity or emergence of a complication may be based on the clinical course and the initial findings. Hypocapnia has been associated with cystic periventricular leukomalacia and should be avoided. Hyperbilirubinemia ^ Although bilirubin is toxic to the central nervous system, the factors that deter mine its toxicity in the infant are many, complex, and incompletely understood. In addition, it is not known whether hyperbilirubinemia can result in chronic neurologic impairment less severe than that caused by kernicterus. Because of limited evidence and individual variations, it is difficult to provide recom mendations suitable to all situations. Follow-up data for apparently healthy term infants with bilirubin concentrations as high as 25 mg/dL (428 micro moles per liter) show no apparent neurologic sequelae. Preterm Infants Kernicterus is rare in preterm infants, and it is controversial whether modest increases of total serum bilirubin result in encephalopathy. Although some observational studies have suggested that bilirubin levels less than or equal to 5 mg/dL (86 micromoles per liter) may cause neurodevelopmental impair ments, others have suggested that modest increases have no such effects. Some published guidelines for the management of jaundice in extremely preterm infants have suggested early phototherapy and exchange transfusion for biliru bin concentrations as low as 10 mg/dL (171 micromoles per liter); however, several studies have failed to confirm a relationship between serum bilirubin concentrations and later neurodevelopmental handicap at concentrations of less than 20 mg/dL (342 micromoles per liter). The guidelines refer to the use of intensive phototherapy, which should be used when the total serum bilirubin level exceeds the line indicated for each category. Infants are designated as higher risk because of the potential negative effects of the conditions listed on albumin binding of bilirubin, the blood-brain barrier, and the susceptibility of the brain cells to damage by bilirubin. These suggested levels represent a consensus of most of the committee but are based on limited evidence, and the levels shown are approximations. During birth hospitalization, exchange transfusion is recommended if the total serum bilirubin level increases to these levels despite intensive phototherapy. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of ges tation. Breastfeeding significantly affects the level and duration of unconjugated hyperbilirubinemia compared with formula feeding, primarily in two ways: 1. It is likely that caloric deprivation and its effect on the enterohepatic circulation of bilirubin is more responsible for this result than dehydration itself. Proper educa tion and support of the mother, together with early and close follow-up after hospital discharge to evaluate the feeding process and the health of the infant, are essential to prevent adverse outcomes. This persistent, mild unconjugated hyperbilirubinemia is caused by a factor in human milk, which is yet unidentified, that promotes an increase in intestinal absorption of bilirubin. This can be combined with phototherapy and will almost always result in a rapid decrease in serum bilirubin concentrations. The mother should be strongly encouraged to maintain lactation and should be provided a breast pump during the period of interrupted nursing. Dehydration and Hyperbilirubinemia Some infants who are admitted to the hospital with high bilirubin concentra tions also may be dehydrated and may need supplemental enteral formula or pumped breast milk, or intravenous fluid, or both. Routine increases in fluid intake are probably not warranted; however, the state of hydration should be carefully monitored. The need for and timing of a repeat noninvasive transcutaneous bilirubin measurement or total serum bilirubin measurement will depend on the age of the infant and the evolution of the hyperbilirubi Neonatal Complications and Management of High-Risk Infants 331 nemia. A noninvasive transcutaneous bilirubin measurement, or total serum bilirubin measurement, or both should be performed if the jaundice appears excessive for the infants age. Risk Assessment Universal predischarge bilirubin screening using total serum bilirubin or transcutaneous bilirubin measurements is recommended to assess the risk of subsequent severe hyperbilirubinemia. Follow-up All hospitals should provide written and verbal information for parents at the time of discharge, which should include an explanation of jaundice, the need to monitor infants for jaundice, and advice on how monitoring should be done. The timing and location of this assessment will be determined by the length of stay in the nursery, risk zone assessed on the appropriate nomogram by plotting the predischarge noninvasive transcutane ous bilirubin level or total serum bilirubin level according to the babys age in hours (see. An increase of the direct serum bilirubin concentra tion always requires further investigation.
In patients for whom there is a high clinical suspicion of disease medications for bipolar disorder trileptal 150mg mastercard, one should proceed to endoscopic evaluation with small bowel biopsy treatment whiplash order trileptal 300 mg visa, and a serologic evaluation treatment by lanshin order 600mg trileptal amex. Note that all testing should be done with patients on a gluten-rich diet for at least several weeks symptoms 10 days before period cheap trileptal online visa, as the mucosal abnormalities may disappear and serologic titers fall after gluten withdrawal from the diet. Referral to a nutritionist may be appropriate, and there are a number of gluten-free foods that are commercially available. Diarrhea is large volume and watery, and is accompanied by paroxysms of flushing and wheezing. A 26-year-old woman who experiences with intermittent abdominal bloating but no diarrhea and is found to have osteopenia and vitamin D deficiency. A 19-year-old college freshman with bulky, foul-smelling, floating stools and excessive flatulence, who has lost 20 lb unintentionally. A thin, 39-year-old man with a family history of celiac disease, who has been adhering to a gluten-free vegetarian diet for the last 3 years, and now complains of gassiness and reflux. A 42-year-old man who was found to have iron deficiency anemia, but has no gastrointestinal symptoms, and recently had a negative colonoscopy. In secretory diarrhea, most of the osmotically active particles are electrolytes, and can be calculated as 2 [Na + K]. The size of osmotic gap (the difference between cal culated and directly measured osmolality) is equivalent to the concentration of the poorly absorbed unmeasured solute in the fecal water. This patient has a stool osmotic gap of 70 (gap >50 is indicative of osmotic diarrhea). Answers C and D are suggestive of carcinoid syndrome and cholera infection, respectively, both causes of secretory diarrhea. Unexplained osteopenia and vitamin D deciency in a young woman, unexplained iron deciency anemia in any patient, and the classic presentation with steatorrhea and weight loss should all be investigated. Empiric treatment with quinolone antibiotics is usually indicated for acute inflammatory diarrhea. Symptoms of malabsorption include greasy, voluminous stools, weight loss, anemia, neurologic disorders from deficiencies of B vitamins, and osteopenia from deficiency of vitamin D and calcium. Adults with undiagnosed celiac disease often present with relatively mild gastrointestinal symptoms, and may only present with unexplained nutritional deficiency (eg, refractory iron deficiency anemia). On examination, her blood pressure is 130/85 mm Hg, heart rate 80 bpm, and weight 285 lb. Laboratory work, typically negative for inflammatory arthritis, and x-rays will confirm the diagnosis. The most important features are the gradual onset, the lack of active synovitis, and the fact that her symptoms worsen with activity. If there were evidence of inflammation or joint effusion, then the best next step would be to aspirate the fluid from the joint and send it for various studies, including Gram stain and culture to assess for infection, crystal analysis to assess for gout or pseudogout, and cell count to assess for inflammation. There may be some crepitus (creaking sound) in the joint, and, unlike inflammatory arthritis, there is often no or minimal tissue swelling (except in the most advanced disease). Other characteristics seen on x-rays include joint space narrowing, subchondral sclerosis, and subchondral cysts. Periarticular pain that is not reproduced with passive motion suggests bursitis or tendonitis. Prolonged pain lasting for more than 1 hour points toward an inflammatory arthritis. Intense inflammation suggests one of the microcrystalline diseases (gout/ pseudogout) or infectious arthritis. Systemic constitutional symptoms, such as weight loss, fatigue, fever, anorexia, and malaise, indicate an underlying inflammatory condition, such as polymyalgia rheumatic, rheumatoid arthritis, systemic lupus erythematosus, or a malignancy, and generally demand aggressive evaluation. Encourage the patient to stay active, because not using the joint can cause further immobility. Multiple short periods of rest throughout the day are better than one large period. Other methods of unloading an osteoarthritic joint include canes and walkers, which can reduce joint forces at the hip by as much as 50%. Equipment such as canes and/or walkers are helpful for patients with advanced disease because these patients are less stable and, as a result, have frequent falls. Physical therapy in the form of heat applied to the affected joints in early disease often is helpful. Perhaps the most important intervention is having the patient maintain full/near-full range of motion with regular exercise. Moist superficial heat can raise the threshold for pain, produce analgesia by acting on free nerve endings, and decrease muscle spasm. Pharmacotherapy early in the course of the disease consists primarily of acetaminophen, the mainstay of therapy. Most findings suggest that glucosamine and chondroitin have little benefit in patients with osteoarthritis. There appear to be few risks associated with their use, however, so patients who wish to try those remedies can be advised that they appear to be relatively safe. Although they are associated with less gastroduodenal toxicity, concerns about an increased risk of cardiovascular adverse events has limited their use. Intra-articular steroids may be rarely useful for long-term treatment and can be helpful for the rare inflammation of a loose cartilage fragment, which may cause the joint to lock up. Improvement throughout the day after approximately 1 to 2 hours of unfreezing the joint Match the following disease processes (A-F) to the clinical setting described in Questions 56. Degenerative joint disease is a major cause of decreased functional status in elderly patients and requires ongoing treatment and evaluation by the physician to try to improve symptoms and to promote mobility. Gouty arthritis often affects the rst metatarsophalangeal joint and can be precipitated by various foods or alcohol. Cervical discharge and inammatory joint are consistent with gonococcal arthritis, which can also present as a migratory arthritis. Acetaminophen is the rst agent of choice in the treatment of early osteoarthritis. Pain in osteoarthritis is worsened with activity and is not associated with morning stiffness. Joint replace ment for severe osteoarthritis is reserved for patients with intractable pain despite medical therapy and for those with severe functional limitations. He became diaphoretic and began to experience chest pain, similar to that of his recent myocardial infarction. Coronary angiography performed prior to discharge revealed no significant coronary artery stenosis. His blood pressure is 124/92 mm Hg while lying down but drops to 95/70 mm Hg upon standing. His neck veins are flat, his chest is clear to auscultation, and his heart rhythm is tachycardic but regular, with a soft systolic murmur at the right sternal border and an S4 gallop. His abdomen is soft with active bowel sounds and mild epigastric tenderness, but no guarding or rebound tenderness, and no masses or organomegaly are appreciated. Rectal examination shows black, sticky stool, which is strongly positive for occult blood. He is tachycardic and has orthostatic hypo tension, likely indicating significant hypovolemia as a result of blood loss. Rather than being a primary problem with his coronary arteries, such as thrombosis or vasospasm, the cardiac ischemia is likely secondary to his acute blood loss and consequent tachycardia and loss of hemoglobin and its oxygen-carrying capacity. For a slowly developing, chronic anemia in patients with good cardiopulmonary reserve, symptoms may not be noted until the hemoglobin level falls very low, for example, to 3 or 4 g/dL. For patients with serious underlying cardiopulmonary disease who depend on adequate oxygen-carrying capacity, smaller declines in hemoglobin level can be devastating. Such is the case with the man in this clinical scenario, who is suffering a cardiac complication as a consequence of his anemia, in this case, unstable angina. He has been treated with medical manage ment, including dual antiplatelet therapy with aspirin and clopidogrel. In this case, it is more likely that his angina is secondary to the acute drop in hemoglobin rather than new cardiac disease. In this case of secondary angina, the anemia must be corrected, which requires an understanding of transfusion medicine. Anemia is generally considered to be a hemoglobin level less than 12 g/dL in women or less than 13 g/dL in men.
Purchase trileptal with american express. Mono The Kissing Disease is a Strain of The Epstein Barr Virus.
Syndromes
- Vitamin B12 level (serum)
- Yellow skin
- A health care provider should do a complete breast exam every year.
- A hole (perforation) in the eardrum
- Exercise may help prevent obesity, and it helps people with diabetes control their blood sugar.
- Electromyography
- Hemolytic-uremic syndrome (HUS), a form of kidney failure with anemia and clotting problems
- National Library Service for the Blind and Physically Handicapped - www.loc.gov/nls
- Nephrotic syndrome