
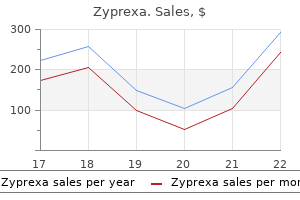
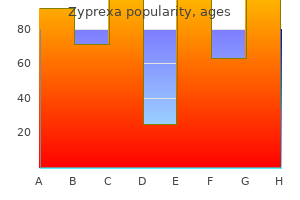
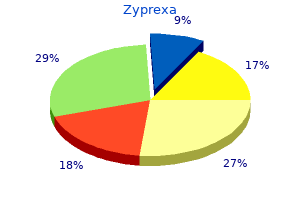
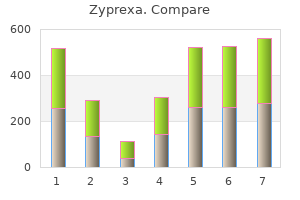
Zyprexa

Lisandro Piaggio, MD
- Pediatric Urologist and Chief, Division of Pediatric Urology,
- Hospital Italiano de Buenos Aires, Buenos Aires, Argentina
Often medicine 5325 order zyprexa 7.5 mg with visa, it is combined with cystoscopy [286 medicine lodge ks purchase 5mg zyprexa free shipping, 287] and/or proctoscopy to help identify the site of multi-compartment pain medicine 750 dollars cheap 20mg zyprexa. Psychological considerations around laparoscopy Three very different studies of laparoscopy suggest that it can improve pain through resolving concerns about serious disease [288] symptoms pregnancy zyprexa 7.5 mg low cost, although showing women the photograph of their pelvic contents did not improve on explanation alone [289]; and integrating somatic and psychological assessment from the start rather than dealing with psychological concerns only after excluding organic causes of pelvic pain [290] crohns medications 6mp order cheap zyprexa line. The scar ruptures with increasing bladder distension chapter 7 medications and older adults cheap zyprexa online amex, producing a characteristic waterfall type of bleeding. Biopsies are helpful in establishing or supporting the clinical diagnosis of both classic and non-lesion types of the disease [160, 187, 296, 299, 300]. Important differential diagnoses to exclude, by histological examination, are carcinoma in situ and tuberculous cystitis. Psychology Anxiety about pain, depression and loss of func on, history of nega ve sexual experiences. Neurological Neurological tes ng during physical examina on: sensory problems, sacral reexes and muscular func on. Tender muscle Palpa on of the pelvic oor muscles, the abdominal muscles and the gluteal muscles. Primary dysmenorrhoea classically begins at the onset of ovulatory menstrual cycles and tends to decrease following childbirth [285]. Secondary dysmenorrhoea suggests the development of a pathological process, such as endometriosis [284], adenomyosis [301] or pelvic infection, which need to be excluded. Bacterial and viral genital tract pathogens should also be excluded [302], as they can cause severe pelvic/vaginal/vulvar pain [303] and are associated with ulcerating lesions and inflammation, which may lead to urinary retention [304]. If there is any doubt about the diagnosis, laparoscopy may be helpful, as one of the differential diagnoses is endometriosis. Endometriosis and adenomyosis the incidence of endometriosis is rising in the developed world. The precise aetiology is unknown, but an association with infertility is recognised [307]. A diagnosis is usually made when a history of secondary dysmenorrhoea and/or dyspareunia exists. On examination, there is often tenderness in the lateral vaginal fornices, reduced uterine mobility, tenderness in the recto-vaginal septum, and on occasion, adnexal masses. Gynaecological malignancy the spread of gynaecological malignancy of the cervix, uterine body or ovary will cause pelvic pain depending on the site of spread. There is often a transient problem with oestrogen deficiency in the post-partum period and during breastfeeding, which can compound this situation. Prolapse is often a disease of older women, and it is often associated with post menopausal oestrogen deficiency, which may lead to pain associated with intercourse. Although they may have a role in supporting the vagina, they are also associated with several complications including bladder, bowel and vaginal trauma [315]. In a subset of these patients, chronic pain may ensue, because mesh insertion may cause nerve and muscle irritation [312]. Patients should be fully evaluated clinically and may need specialised imaging, using contrast mediums if necessary, to make a diagnosis. Haemorrhoids Chronic pelvic pain is rare in haemorrhoidal disease because endoscopic and surgical treatment is mostly effective in acute disease. Haemorrhoidal pain on defecation associated with bleeding is usually due to prolapse or ulceration of internal haemorrhoids. Anaemia from haemorrhoidal bleeding is rare but may arise in patients on anti-coagulation therapy, or those with clotting disorders. Anal fissure Anal fissures are tears in the distal anal canal and induce pain during and after defecation. Persistence of symptoms beyond six weeks or visible transversal anal sphincter fibres define chronicity. Proctitis Abdominal and pelvic pain in patients with inflammatory bowel disease and proctitis are often difficult to interpret. Faecal calprotectin may help to differentiate between inflammation and functional pain, to spare steroids. Use a validated symptom and quality of life scoring instrument, such as the National Strong Institutes of Health Chronic Prostatitis Symptom Index, for initial assessment and follow-up. Assess prostate pain syndrome associated negative cognitive, behavioural, sexual, Strong or emotional consequences, as well as symptoms of lower urinary tract and sexual dysfunctions. Use a validated symptom and quality of life scoring instrument for initial assessment and Strong follow-up. Refer to a gynaecologist if clinical suspicion of a gynaecological cause for pain following Strong complete urological evaluation. Recommendations Strength rating Rule out confusable diseases, such as neoplastic disease, infection, trauma and spinal Strong pathology. If a peripheral nerve pain syndrome is suspected, refer early to an expert in the field, Weak working within a multi-disciplinary team environment. Imaging and neurophysiology help diagnosis but image and nerve locator guided local Weak anaesthetic injection is preferable. Strong Ask patients what they think is the cause of their pain to allow the opportunity to inform Strong and reassure. Strong In patients with chronic pelvic pain syndrome it is recommended to actively look for the Weak presence of myofascial trigger points. Single interventions rarely work in isolation and need to be considered within a broader personalised management strategy. Pharmacological and non pharmacological interventions should be considered with a clear understanding of the potential outcomes and end points. These may well include: psychology, physiotherapy, drugs and more invasive interventions. Additional written information or direction to reliable sources of information is useful; practitioners tend to rely on locally produced material or pharmaceutical products of variable quality while endorsing the need for independent materials for patients [320]. Information improves adherence to treatment and underpins self-management, as shown in many other painful and non-painful disorders but not specifically in pelvic and abdominal pain except by a small qualitative study [321]. In most studies that have been done looking at the effect of physiotherapy in pelvic pain, the treatment of the pelvic floor is only part of the pain management. In a review about physiotherapy in women with pelvic pain, it was concluded that recommendations for physiotherapy should be given with caution [322]. One of these three found that Mensendieck somatocognitive therapy showed a pain reduction after one year follow up of 64%. In the prostate pain group, there was no difference between the two treatment arms. In the bladder pain group, myofascial treatment did significantly better than the massage. The fact that the prostate pain group consisted of only men is mentioned as a possible confounding factor [324]. Myofacial trigger point release Treatment of myofascial trigger points can be done by manual therapy, dry needling and wet needling. The evidence for all the different treatments is weak, with most studies showing no significant difference between these techniques, though most studies were small and heterogeneous with regards to the patients and methods. There is no evidence that manual techniques are more effective than no treatment [325]. Different systematic reviews have come to the conclusion that, although there is an effect of needling on pain, it is neither supported nor refuted that this effect is better than placebo [326]. Other reviews have concluded that the same is true for the difference between dry and wet needling [327, 328]. Each trigger point was identified by intravaginal palpation and injected with bupivacaine, lidocaine and triamcinolone. Seventy-two percent of women improved with the first trigger point injection, with 33% being completely pain-free. As previously described in dyssynergic defecation, the ability to expel a 50 mL water filled balloon and to relax pelvic floor muscles after biofeedback treatment were predictive of a favourable therapeutic outcome [147]. The pathophysiology of the chronic anal pain syndrome is therefore similar to that of dyssynergic defecation, and this favours the role of the pelvic floor muscles in the pathophysiology of both conditions. Specific behavioural strategies for women who have urogenital complaints and female sexual dysfunction often include exploring alternatives to sexual intercourse (manual or oral pleasuring), different coital positions (female superior or side lying), and pacing, such as limiting thrusting to less than that causes pain. Planning for the time of intercourse is important, and scheduling a clinic visit after intercourse might be useful to identify specific sites and causes of post-coital flares. Other behavioural changes involve pre and post-coital voiding, application of ice packs to the genital or suprapubic area [333, 334], and use of vaginal dilators before penile penetration. In patients with an overactive pelvic floor, referral for physical therapy, myofascial release, and internal pelvic floor muscle massage may offer relief [336]. In uncontrolled studies significant symptomatic improvement has been reported from heat therapy, for example, transrectal and transurethral thermotherapy [338, 339]. A small sham-controlled double-blind study of four times weekly perineal extracorporeal shockwave therapy (n=30) in men with chronic pelvic pain syndrome showed significant improvement in pain, QoL, and voiding compared to the control group (n=30) over twelve weeks [340]. Two other randomised sham-controlled studies, have been published more recently, one comparing ten treatment sessions over two weeks (n=40 vs. Unfortunately, no long term effects at 24 weeks could be shown in a published follow-up study of the second [343]. Two systematic reviews and meta-analyses have been published in 2016 analysing seven randomised-controlled studies on a total of 471 participants comparing acupuncture to sham control or oral medical treatment [346, 347]. Furthermore, rigorous trials should be undertaken to provide some clarity for a commonly used intervention. Ideally, treatment follows general principles and practice in the field of chronic pain [350, 351], but these have been neglected in pelvic pain. Two systematic reviews and meta-analyses of the few heterogeneous trials of psychologically based treatment for pelvic pain [352, 353] found some short-term benefits for pain, of around 50%, comparable to that from pharmacotherapy, but this was not sustained at follow-up. The importance of multi-disciplinary treatment is emphasised by several reviews [43, 359, 360], and the need for high quality psychological treatment evaluation is underlined [359]. For less disabled and distressed patients, this can be delivered in part over the internet [361]. Several other reviews make positive comments on psychological involvement [362], and recommend addressing psychological concerns from the outset, directed at the pain itself, with the intended outcome of reducing its impact on life [34], or at adjustment to pain, with improved mood and function and reduced health-care use, with or without pain reduction [36]. A good model of such an intervention, albeit a pilot study, is by Tripp et al [363] for men with chronic pelvic pain. Where there is no evidence the reader is directed to the section on analgesics below (5. There is a large discrepancy in the treatment effects reported in case series and controlled trials that results from a large placebo effect or publication bias. One strategy for improving treatment effects may be stratification of patient phenotypes. Anti-inflammatory drugs were 80% more likely to have a favourable response than placebo. Overall, a moderate treatment effect has been shown for anti-inflammatory drugs, but larger studies are needed for confirmation, and long-term side-effects have to be taken into account. Whereas one systematic review and meta-analysis has not reported a relevant effect of blockers due to study heterogeneity [373], another network meta-analysis of blockers [374] has shown significant improvement in total symptoms, pain, voiding, and QoL scores. Antibiotic therapy Empirical antibiotic therapy is widely used because some patients have improved with antimicrobial therapy. Patients responding to antibiotics should be maintained on medication for four to six weeks or even longer. The only randomised placebo-controlled trials of sufficient quality have been done for oral antibiotic treatment with ciprofloxacin (six weeks) [153], levofloxacin (six weeks) [378], and tetracycline hydrochloride (twelve weeks) [379]. Although direct meta-analysis has not shown significant differences in outcome measures, network meta-analysis has suggested significant effects in decreasing total symptom, pain, voiding, and QoL scores compared with placebo. Combination therapy of antibiotics with blockers has shown even better outcomes in network meta-analysis. Despite significant improvement in symptom scores, antibiotic therapy did not lead to statistically significant higher response rates [380]. In addition, the sample sizes of the studies were relatively small and treatment effects only modest and most of the time below clinical significance. If antibiotics are used, other therapeutic options should be offered after one unsuccessful course of a quinolone or tetracycline antibiotic over six weeks. A six-month placebo-controlled study showed a non-significant tendency towards better outcome in favour of finasteride, possibly because of a lack of statistical power [383]. Phytotherapy Phytotherapy applies scientific research to the practice of herbal medicine. In contrast, treatment with saw palmetto, most commonly used for benign prostatic hyperplasia, did not improve symptoms over a one-year period [382]. In a systematic review and meta-analysis, patients treated with phytotherapy were found to have significantly lower pain scores than those treated with placebo [374].
Green Juice Ingredients Materials 1 medium organic cucumber 1 strainer 2 large organic kale leaves Container with a spout head organic parsley 1 cup fltered water or Coconut Water Yields one 16-ounce batch of juice medicine xarelto purchase zyprexa overnight. Double the recipe You may also add 1 carrot if you desire a sweeter fnal for 2 servings product Recipe directions on following page symptoms uti in women zyprexa 2.5mg mastercard. When all produce is liquefed medications osteoporosis discount zyprexa 20mg amex, move blender over sink treatment vitiligo order discount zyprexa on-line, and place a large mouth container with a spout into the sink medicine 257 best purchase for zyprexa. Using a spoon or your hands medicine hat weather order zyprexa 20mg visa, squeeze the liquid out of the strainer into the container. When the liquid is removed and the pulp feels dry, empty the pulp into the garbage. Start the soaking the night before, so the grains will soak at least 7 to 8 hours. After the soaking time has passed, strain the grains and discard the soaking water. All of the grains are easily kept for 2 days in the refrigerator, therefore you can make enough for 2 days worth of breakfast. Store the left-over grains in a glass or ceramic container with a lid or plastic wrap. You can either remove from the refrigerator about an hour before you will eat to enjoy at room temperature, or you can place the grain in a saucepan with 1 teaspoon of water drizzled over the top. Combine your optimal serving size of quinoa in a small pot (use a pot that has a tight-ftting lid) with twice as much water (for 1/3 cup of quinoa, add 2/3 cup of water, for cup of quinoa, add 1 cup of water). Bring the mixture to a boil, then lower the temperature on your stove and simmer, covered, for about 15 minutes, or until the quinoa is tender, but still chewy and a white spiral-like thread appears around each grain. For a nuttier favor, the quinoa can be toasted in a dry skillet for a few minutes before cooking. Combine your optimal serving size of amaranth with three times as much water (for 1/3 cup of amaranth, use 1 cup of water, for cup of amaranth, use 1 cups of water) in a small pot. Amaranth can also be enjoyed with hemp milk and stevia for more of a breakfast cereal-type meal. Your ratio for millet is 2 times the amount of water to your serving size of millet (for 1/3 cup of millet, use 7/8 cup of water, for cup of millet, use 1 1/4 cups of water). For a nuttier favor, the millet can be toasted in a dry skillet for a few minutes before cooking. Unfortunately, the labels on most packaged brown rice recommend an ineffective method that suggests boiling water and rice in a two-to-one ratio, then allowing the mixture to simmer for 40 minutes or more, until all the liquid is absorbed. We followed those directions and ended up throwing away more than a few pots of unsatisfying rice. What we ultimately found is that brown rice looks and tastes the best when it has been boiled and drained like pasta and then is steamed in the small amount of moisture that remains in the pot. The boiling cooks the rice, while the subsequent steaming allows the grains to retain their integrity and come out light and fuffy. Bring 12 cups water to a boil in a large pot with a tight ftting lid over high heat. Here are some of our favorite recipes that are tasty and will help you stay on track. Rice Flour Pancakes Ingredients Directions 1 cup rice four Sift the rice four, sugar, baking powder and salt together in 1 tbs sugar a bowl. Beat in the rice milk or soy milk until the mixture has 2 tsp baking powder a smooth consistency. Add the beaten egg and olive oil or tsp salt vegetable oil and mix until just blended. Salt and pepper oz low-fat spread or butter Whisk the egg whites until they stand in soft peaks. Grated low-fat cheese optional Whisk the egg yolks with the cold water until pale and creamy and season. Melt the low fat spread in the omelette pan, pour in the omelette mixture and level the top. Sprinkle with cheese, if using, and place under the grill for approximately minute, until cheese begins to melt. Add the clam broth and the 3 cups clam broth rice milk and whisk the mixture until it is smooth. Bring the soup to a boil, 1 tbs chopped parsley cover and reduce the heat to a simmer. Place the chicken cubes in a medium bowl and drizzle with olive oil and lime, toss to coat. Line a baking sheet with foil and broil the skewers for 4-5 minutes on each side, depending on how hot your broiler is and how large you cut the chicken. Place sorbet in a sealed container and place in the freezer for 2 hours before serving. Historically, the care of this group of patients has been underfunded and overlooked and there has been resultant variability in the quality of care provided. Adoption of these improvements is still patchy and Commissioners can play a very positive role in encouraging service improvement. Resource allocation in the past has not reflected the complexity of such cases, and there is significant variability in survival between units. Adequate consultant input, routine critical care, adequate and timely theatre access and a defined rota for interventional radiology are all key components of the best services. The development of acute ambulatory surgical services can reduce admissions within this basket of diagnoses by up to 30% and thereby reduce costs. The presence of a defined acute biliary pathway can help identify well organised services. Predicated theatre access is required if this service is to be delivered reliably. They represent a strong audit tool, both for commissioners and individual Trusts, to benchmark their results. The care of this vast, heterogenous group of patients is beset with challenges, not least because this is an area that has traditionally been underfunded and overlooked. Data from the Emergency Laparotomy Network confirm that emergency laparotomy still carries a mortality of 2 15% overall with even higher risks in the elderly and comorbid. Critical care resource allocation in the past has not reflected the complexity of such cases, and there is significant variability in outcomes between units. At the other end of the spectrum, around 90, 000 patients annually are admitted with non-specific abdominal pain, where no further diagnosis is forthcoming. Along with sub-acute conditions such as cholecystitis (where patients may wait up to a week for surgery), these represent a substantial, expensive and potentially avoidable, inpatient burden. There is an appetite for service improvement and innovative ways of managing the acute surgical take are fast being developed. This guide for commissioners outlines evidence-based best practice in the management of acute abdominal pain. It is not intended as a comprehensive guide to all emergency surgical conditions, and reference is made to other bodies where a standard has already been set. This document defines high quality, safe and cost effective management of acute abdominal pain, which, if followed, will result in improved outcomes and patient experience. The vast majority of patients with abdominal pain are effectively managed in general practice. Acute pain of less than 24 hours duration and localised peritonism are the strongest predictors of the need for 3 secondary care referral. Of those who are referred to secondary care, there will be a proportion that, after senior surgical assessment, are discharged immediately or managed in an ambulatory setting. Different care models in Europe appear to allow more effective primary and emergency care management. Secondary care History and examination the provision of an experienced surgeon (at registrar level or above) to take referrals, divert to other 4 specialties and provide early assessment has been shown to reduce unnecessary admission. In larger units it may prove cost efficient to alter or augment the traditional on call team structure. There is some evidence 5-7 that formally structured patient data sheets improve diagnostic accuracy. The use of opiate analgesia in acute abdominal pain is beneficial in terms of patient comfort, and does not 8 delay diagnosis or retard decision making. Digital rectal examination has been shown to have a low utility in the diagnosis of undifferentiated 9 abdominal pain, and should be used selectively in those presenting with colonic symptoms. Arterial blood gases (including estimation of lactate) are essential in the evaluation of abdominal catastrophe. An erect chest radiograph remains the primary investigation of choice for the detection of free intraperitoneal gas, and may detect lower lobar pneumonia. Plain abdominal radiography should be used selectively in the event of suspected intestinal obstruction, 10 fulminant colitis, or perforation. Seven day access to ultrasound is required, with dedicated slots for emergency surgical admissions. There are 5 Commissioning guide 2014 Emergency general surgery relatively few occasions where a patient cannot be stabilised sufficiently for scanning to take place, and the information afforded in terms of accurate diagnosis and therapeutic intervention cannot be underestimated. Criteria for admission All patients with acute pancreatitis, intestinal obstruction, or abdominal sepsis will require admission. Those with uncomplicated diverticulitis can be discharged on oral antibiotics or managed in an ambulatory setting where such facilities exist. Those with suspected biliary colic or uncomplicated cholecystitis are suitable for early discharge or ambulatory care, as are younger patients with non-specific abdominal pain, in the absence of any derangement in inflammatory markers. The substantial associated mortality is particularly striking when compared to major elective colorectal resection which 14 carries an average mortality of 4. Emergency outcomes vary three fold between units giving a real 7 Commissioning guide 2014 Emergency general surgery 53 opportunity for better outcomes and reduced cost. There is a shortfall particularly in access to critical care beds for one third of these 55 patients, in operating theatre access and to interventional radiology. Approximately 50% of surgeons 55, 15, 16 describe delays in theatre access for emergency cases and interventional radiology is now an optimal emergency treatment for some conditions. Management of complications among major elective cases also varies substantially and survival 57 differs significantly (two fold) between best and worst units 2 c. Consultant involvement in high risk cases is suboptimal being reduced at night with sicker cases In line with many other disciplines, there is a current re-evaluation of major general emergency care to determine which aspects of intervention should be centralised or delivered by specialists. Assessment should remain a general skill delivered as close to home as possible: clinical pathways which meet current standards should feature early senior surgical assessment and direct patients to timely specialist care when required. A national audit of emergency laparotomy has begun with patient outcome data available from April 58 2015. Critical care teams should be 17 involved peri-operatively, where possible, to ensure optimal safe care. Is always undertaken with consultant surgeon and consultant anaesthetist present b. Is performed within the following maximum recommended timings deferring elective or less urgent cases when necessary i. Background 19 Emergency ambulatory care is well established in medicine but not yet within surgery. Pilot studies have shown that up to 30% of patients on a general surgical emergency take can be managed in this way. Further development of this type of service will be common place in the next three years. Assessment Given the risk associated with a surgical ambulatory pathway the initial assessment should be made by a consultant surgeon. It is generally defined as acute abdominal pain of less than seven days duration, where no diagnosis is reached after examination and baseline investigations. However general anaesthetic and laparoscopy are associated with a small risk of complication and performing this procedure specifically for the diagnosis of a non-surgical condition is controversial. Appropriate history taking and counselling of those with functional bowel disorders may avoid unnecessary laparoscopy. The lifetime risk 24-26 of having appendicitis is 7% 8% with an overall incidence of 11 cases per 10, 000 population per year. Whilst in some patients, who present with a typical history and convincing examination signs, it is easy to determine what their management should be, those with less specific signs can be more of a diagnostic challenge. It is these patients that require further time and investigations to determine the correct diagnosis and subsequent treatment.
Nat Rev resistance symptoms 3 days dpo purchase generic zyprexa on-line, there is low proporton of Firmicutes but a higher Microbiol 11: 277-284 treatment of hemorrhoids cheap zyprexa 7.5 mg with amex. Targetng of specifc consttuents of microbiota treatment to prevent preterm birth in women with previous may potentally permeate removal of harmful microorganisms preterm delivery treatment non hodgkins lymphoma discount zyprexa 20mg with visa. Placental viral infectons sensitzes to endotoxin-induced preterm labor: a double hit hypothesis medicine naproxen order 7.5mg zyprexa overnight delivery. Wang H medicine qhs order zyprexa 2.5mg on-line, Hirsch E (2003) Bacterially-induced preterm labor and the authors declare that they have no competng interests medicine queen mary buy 2.5 mg zyprexa with mastercard. Nat Rev Immunol 4: in the female genital tract during pregnancy: Tolerance versus 219-232. Science 349: to bacteria and is targeted by virus: Mechanism of polymicrobial 1101-1106. Host-microbe interactons in distal airways: relevacnce to (2015) Early infancy microbial and metabolic alteratons afect chronic airway diseases. Am J Respir expression of antmicrobial peptdes and proinfammatory Crit Care Med 186: 536-545. Ann Am cell wall integrity of mycobacteria and pathogenesis of Thorac Soc 11: 964-968. Sekirov I, Russel S, Antunes L, Finaly B (2010) Gut microbiota in (2012) Genomic analysis identfes associaton of Fusobacterium health and disease. Brint E, Macsharry J, Fanning A, Shanahan F, Quigley E (2011) microbiota in western infants. Diferental expression of toll-like receptors in patents with irritable bowel syndrome. Tremaroli V, Backhed F (2012) Functonal interactons between the gut microbiota and host metabolism. Ghoshal U, Shukla R, Gwee K, Ng S, Quigley F (2012) the gut microbiota and irritable bowel syndrome: friend or foe Claesson M, Cusack S, Osullivan O, Greene-Diniz R, de Weerd H, signatures in fecal samples from patents with irritable bowel et al. Manichanh C, Borruel N, Casellas F, Guarner F (2012) the gut analysis in humanized gnotobiotc mice. Proteus species pos sess many virulence factors potentially relevant to gastrointestinal pathogenicity, including motility; adherence; the production of urease, hemolysins, and IgA pro teases; and the ability to acquire antibiotic resistance. Most Pcommonly, they are recognized clinically as a cause of urinary tract infections. As a result, their detection in disease states using 16S proling, and possibly metagenomics, may have rendered Proteus spp. This review aims to provide an overview of the genus Proteus in terms of its known virulence factors as well as to collate the evidence surrounding the role of Proteus spp. The rst isolates were reported and characterized by Hauser in the late 19th century (5). Other genera within the Enterobacteriaceae family, such as Escherichia, Shigella, Salmonella, and Klebsiella, have received due attention in this regard, while Proteus has not been comprehensively investigated. Swimmer cells predominate in liquid environments as single cells with 4 to 10 peritrichous agella. When Proteus cells are placed in a viscous environment or on a solid surface, they undergo differentiation to lamentous, multinucleated, highly agellated swarmer cells. Following this differentiation, a consolidation phase occurs, where the cells revert to a shorter morphotype, and metabolic preparation occurs prior to the next swarming cycle (18). Proteus mirabilis undergoes swarming differentiation at much higher concentrations of agar (1. In vivo, swarmer cells have been demonstrated in mouse models of ascending urinary tract infection only infrequently, with the occasional swarmer cell being isolated from the kidneys and bladder stones of infected mice (22, 23). The swarming phenotype can occur under both aerobic and anaerobic conditions (24) and can be induced by the concentration of amino acids, in particular July 2018 Volume 31 Issue 3 e00085-17 cmr. Swarming has been shown to be an important factor in intracellular invasion and persistence, with 15 to 20-fold more swarmer cells than swimmer cells being capable of the intracellular invasion of uroepithelial cells (30). There is some evidence that swarming Proteus strains are more invasive in urinary tract mouse models than are swarm-defective mutant strains (22). While we cannot yet conclude denitively that swarming behavior occurs in the gut in vivo, the combination of a viscous surface (such as the gut mucosa), the high availability of glutamine and polyamines such as putrescine (26, 31, 33), and electron acceptors for anaerobic respiration such as choline (32) makes it likely that the gut environment may be permissive for swarming. Adhesion to epithelial surfaces is essential for the pathogenesis of Proteus infections in both the urinary and gastrointestinal tracts. These mbriae and adhesins play a major role in the formation of bacterial biolms, a common complication of both urinary and gastrointestinal instrumentation (37). A comparison of the 17 individual chaperone-usher mbrial operons across the 7 sequenced P. Of these, it is likely that at least two, and up to six, of the characterized mbriae can be assembled on the cell surface at any one time (36, 42). The regulation of motility and the expression of adhesion factors are tightly coupled; of the 17 mbrial operons, at least 10 gene clusters possess a homolog of the mrpJ gene, a repressor of motility (43). The adaptation of Proteus species to mucosal surfaces by way of both mbrial expression (for adherence) and swarming motility could increase the invasiveness, persistence, and pathogenicity of these species in the gut (Table 1 and. The urease enzyme is a microbiological adaptation to metabolize urea, the most abundant nitrogenous waste product of human metabolism (46). Urease gener ates ammonia and carbonic acid as end products, with this ammonia providing a rich source of nitrogen for microbial metabolism in the gut (47). Urease confers a survival advantage to Proteus by providing nitrate for nonfermentative anaerobic respiration. This in turn promotes the population expansion of the Enterobacteriaceae (including Proteus)(48, 49). Additionally, as with Helicobacter pylori, the presence of this enzyme likely confers a survival advantage through increasing the local pH of the environment, allowing urease-positive organisms to survive in more-acidic environments such as the July 2018 Volume 31 Issue 3 e00085-17 cmr. The Proteus genus produces two distinct cytotoxic hemolysins, HpmA and HlyA (51, 54, 55). HpmA has been shown to lyse erythrocytes, bladder epithelial cells, B-cell lymphoma cells, and monocytes, while HlyA can lyse erythrocytes, broblasts, and neutrophils (55, 56). HpmA is a cell-associated hemolysin, encoded on the hpm locus along with HpmB (an activator and chaperone of HpmA). The expression of these hemolysin proteins is tightly coupled to the swimming-swarming cycle, with swarming cells being 18-fold more cytotoxic than swimmer cells (30). HpmA has also been shown to lyse erythrocytes under anaerobic conditions and at multiple temper atures (58). Intracellular invasion by Proteus mirabilis has been assessed mainly by using cellular invasion assays in cell lines ranging from uroepithelial cells to colonic cell types. After the invasion of uroepithelial cells, swarmer cells start to divide, develop septums, and differentiate back to an average of 50 to 300 swimmer cells within the cytoplasm (30). There are differences in the intracellular invasion and uptake pathways depending on the cell type, with intracel July 2018 Volume 31 Issue 3 e00085-17 cmr. These mechanisms may contribute to effective intracellular colonization (cytoplasmic colonies), evasion of the host immune system, and resistance to antibiotics (60). Proteus mirabilis is a common cause of pathogenic infection of bladders augmented with bowel segments (enterocystoplasty). Proteus mirabilis has many invasive characteristics; however, they remain to be directly char acterized in the context of gastrointestinal disease. This enzyme has a key role in the evasion of innate immune destruction by Proteus species by the proteolytic digestion of secretory IgA, IgG, and other cellular components in the urinary and gastrointestinal tracts (20, 21). The expression of this protein has been shown to be correlated tightly with cellular differentiation from swimmer to swarming cells by P. ZapA hydrolyzes human defensin 1, a constitutively expressed innate immune antimicrobial peptide that is expressed in the colonic epithelium, as well as secretory IgA (20, 21). The expression of ZapA in the gut may provide a survival advantage to Proteus spp. As a Gram-negative pathogen, Proteus species possess intrinsic characteristics similar to those of other Enterobacteriaceae, such as Escherichia coli and Salmonella enterica serovar Typhimurium, including the production of agellin July 2018 Volume 31 Issue 3 e00085-17 cmr. Approximately 80 O-antigen serogroups have been reported, derived from a total of 60 O-antigen gene clusters (11, 73). Antibodies to O-antigens are not uncommon in human sera, for example, 25% of blood donors have anti-P. The expression levels of virulence factors, such as urease, proteases (ZapA), and hemolysin, can vary signicantly between the O-antigen serogroups, with negatively charged O-polysaccharide serogroups having higher ureolytic, proteolytic, and swarming activities (75). In addition, bacterial agellins, the repeating protein subunits from which agella are built, are highly immunogenic due to their three-dimensional structure (76). Bac terial agellin is sensed by Toll-like receptor 5, which activates a number of downstream inammatory pathways, including MyD88 (72, 76, 77). Recombination of the agellin genes aA and aB, leading to hybrid agellin proteins with signicant antigenic variation, also contributes to innate immune evasion by Proteus spp. They also possess intrinsic resistance to colistin, tigecycline, and tetracycline (82). While most species of Proteus remain sensitive to a range of antibiotics, increasing rates of acquired antibiotic resistance in the Enterobacteriaceae are a growing problem (83). In gastrointestinal disease, the antibiotic sensitivity prole of Proteus species is relevant to pathogenicity under conditions that may be exacerbated by antibiotic perturbation of the gut microbiome. Clinical Microbiology Reviews Vaccine Candidates A full review of the treatment of Proteus infection is outside the scope of this review. There has been success by using the intranasal delivery of MrpH, the mbrial tip adhesin of P. A fusion protein comprised of MrpH and mannose-binding protein delivered intranasally provided 75% protection from P. A clinical study of an inactivated bacterial cell suspension of four bacterial species, including a strain of P. Infants from Sweden and Pakistan were assessed for Enterobacteriaceae based on mode of delivery (vaginal versus cesarean) and breastfeeding behavior (91). Cesarean births in Pakistan were associated with Proteus species colonization within 3 days, with 11 of 21 cesarean delivered and 1 of 9 vaginally delivered infants being positive for Proteus spp. Proteus species were present in 8% of gastric samples, 46% of duodenal and jejunal samples, 19% of ileal samples, 13% of cecal samples, and 38% of samples from the transverse colon (12). Muller compared the recovery of Proteus species from the stool specimens of 1, 422 healthy subjects. A smaller culture-based study of 60 patients with gastrointestinal symptoms who tested negative for parasites demonstrated a colonization rate of 33% (20/60 patients) for P. In a study of multiple drug-resistant Gram-negative bacteria in the rectum of long-term-care patients, 52 drug-resistant strains were identied, 15 of which were P. However, that study did not take into account the possible administration of antibiotics to affected patients or the potential bystander or overgrowth effect (92). When three clinical isolates were compared to four local and reference strains of P. In summary, Proteus species can be linked to diarrheal states, but their primary pathogenic role has not been conrmed. In 13 infants with feeding tubes without gastrointestinal symptoms, Proteus was isolated from the throat in 8% of patients, from the gastric juice in 15% of patients, and from the duodenal uid in 8% of patients (98). Association with Hepatobiliary Disease Early culture-based surveys of patients undergoing biliary surgery showed the occasional isolation of Proteus species from the biliary tract (13% of bile samples) (102). In a metagenomic analysis using multitag pyrosequencing, the rectosigmoid mu cosal community of healthy individuals was compared with that from patients with cirrhosis. Patients with cirrhosis had an elevated proportion of Proteus species com pared with controls; the relative abundance in healthy controls was 0. In a series of patients undergoing liver resection, Proteus vulgaris bacteremia was identied in two patients, and polymicrobial infections were identied in eight patients (106). Implantable devices, such as stents, are also at risk of colonization and biolm forma tion (107). Pancreatic Disease There are isolated reports of Proteus species infections of the pancreas, including a patient with a large infected pancreatic pseudocyst compressing the common bile duct. The cystic contents were polymicrobial, including Proteus vulgaris, Morganella morganii, Stenotrophomonas maltophilia, and Pseudomonas aeruginosa (108). Clinical Microbiology Reviews Intestinal Disease There are a number of reported links between Proteus spp. A small study of the downstream effects of small bowel ulceration caused by nonsteroidal anti-inammatory drugs in rats identied a mixed population of E. When treated with metronidazole, rats were protected from ulcer devel opment (109). Viable bacterial translocation of Proteus mirabilis across the intact intestinal barrier has been demonstrated from the cecal and colonic mucosa of a monoassociated mouse model, with bacteria being additionally isolated from the mesenteric lymph nodes and the liver (111).
Buy discount zyprexa 7.5mg. IV Hydration Treats Symptoms of Dehydration in Nashville.
Lukashevich V treatment yeast infection men purchase zyprexa line, Del Prato S medications knee buy zyprexa 20 mg otc, Araga M medicine 4212 proven zyprexa 10mg, Kothny W (2014) Efficacy ble-blind medications covered by medi cal purchase zyprexa with american express, placebo-controlled trial treatment xanax withdrawal generic 20mg zyprexa visa. Wang C treatment 002 order generic zyprexa on-line, Mamza J, Idris I (2015) Biphasic vs basal bolus insulin extension to a 26-week main trial. Anyanwagu U, Mamza J, Gordon J et al (2017) Premixed vs plus lixisenatide, versus insulin glargine and lixisenatide basal-bolus insulin regimen in type 2 diabetes: comparison of monocomponents in type 2 diabetes inadequately controlled on clinical outcomes from randomized controlled trials and real oral agents: the LixiLan-O randomized trial. Aronson R, Reznik Y, Conget I et al (2016) Sustained efficacy of safety of LixiLan, a titratable fixed-ratio combination of insulin insulin pump therapy compared with multiple daily injections in glargine plus lixisenatide in type 2 diabetes inadequately con type 2 diabetes: 12-month data from the OpT2mise randomized trolled on basal insulin and metformin: the LixiLan-L randomized trial. Linjawi S, Lee B-W, Tabak O et al (2018) A 32-week randomized Internet Res 17:e86. Kernan & Chantal Mathieu & 7, 8 9, 10 11 12, 13 14 Geltrude Mingrone & Peter Rossing & Apostolos Tsapas & Deborah J. Ciell, Senior Scientific Advisor the Ideal Protein Weight Loss Protocol is a medically designed protocol that results in rapid fat loss while sparing the lean body mass. This weight loss protocol has been used in well over one thousand medi spas and aesthetical clinics in Canada for the last nine years with great success. Our products are only available for purchase via Ideal Protein clinic partners but are not sold in stores or over the Internet. We are a manufacturer and distributor of high biological value foods and supplements. Our sales team provides complete training, continual education and in-house support free of charge. In addition, our licensed medical professionals (physicians, pharmacists and nurse practitioners) are always available via phone or email to answer clinical questions. Principles Behind the Protocol To lose weight one must obviously consume fewer calories than are expended. However, to specifically target fat loss other factors must be taken into consideration along with a maintenance program, which is completely different than the interventional program. The body has four compartments of energy from which it draws its metabolic needs: 1. First, the body burns the glucose in the blood and then reaches the glycogen reserves. Once the glycogen is exhausted, then and only then, will the body start burning muscle and fat compartments. If we replenish the glycogen the fat burning stops until it is once again depleted. Insulin and glucagon, two master metabolic hormones, mediate how the body shifts from one compartment of energy to the next. Why We Are Successful Any hypocaloric diet based on a balanced diet, will result in weight loss. When these amounts are cut in half (while keeping the ratio of macronutrients the same), we will have a balanced diet with half the calories. Patients or clients will lose weight but there are a few problems with this seemingly logical approach. First, if we continue to replenish some of the glycogen stores daily (60% of calories coming from carbohydrates, most of which will be converted to glucose in vivo) our fat burning will stop until that has been depleted. Second, and more importantly, decreasing the minimal daily requirements of protein will lead to muscle loss. Remember the weight loss program, where two anorectics were used to make patients or clients lose weight but caused extremely dangerous pulmonary and heart problems When patients or clients have achieved their goal weight, what is the predictable result They go back to eating normal size meals but their metabolism is slower and they regain the weight, often times ending up heavier than before. In contrast, the Ideal Protein Weight Loss Protocol takes a different track, for a relatively short time we will use an unbalanced diet. We keep the minimum daily protein requirement the same (roughly 1/2 gram of protein per pound of lean body weight) and build the diet around this. What patients or clients need to understand is that this is not a high protein diet. Next, if we want to lose fat it is logical that we would eliminate most fats from the diet while keeping ample amounts of essential fatty acids. Since we do not want to replace glycogen stores, we keep these at a bare minimum, approximately 30 grams (1 oz. This forces the body to stay in the fat-burning mode 24 hours a day, which is called a ketogenic diet. Our patients or clients will consume four cups of non-starchy vegetables and two green salads daily. The patients or clients will also be given a multi-vitamin, calcium, magnesium, potassium, omega-3 and sea salt to ensure proper electrolyte balance is maintained. We only provide the supplements to replace the food groups that we are temporarily taking away. Ideal Protein has also developed an Alternative Plan which is suitable for Type I diabetics. This program is similar to the ketogenic method except that we give a dairy, fruit and grain serving every day to prevent the diabetic patient or client who wishes to follow the Ideal Protein Weight Loss Protocol from going into a state of moderate to strong ketosis. Since Type I diabetics do not produce insulin, a risk of ketoacidosis exists and these patients or clients should never be placed on a strong ketogenic diet. Our Foods the highlight of our weight loss protocol is the wonderful variety of protein-based foods the client will consume during the weight loss phases. These are high biological value proteins, containing all nine essential amino acids. This gives the patient or client many options and is designed to accommodate people who are sensitive to dairy, soy or those who are vegetarians by allowing them to participate in the program. Our products are delicious and we currently have over 80 different products including shakes, juices, bars, soups, chili, pancakes, oatmeal, and many more. Our products include hot and cold foods, different textures and range from sweet to salty. The patient or client will use these products to build complete meals, adding vegetables and salads. Each sealed envelope ensures full potency and contains about 18 to 20 grams of protein with very little to no fat or sugar. These are easy to prepare and can be incorporated into a busy lifestyle very easily. Metabolic Syndrome: Insulin Resistance and Hyperinsulinemia Metabolic Syndrome, arguably the epidemic of the century, is the name given to a general disorder characterized by four symptoms: 1. Pharmacological treatment of the symptoms of the Metabolic Syndrome never affects a cure, and many times will exacerbate the symptoms. We commonly prescribe medications to help the pancreas produce even more insulin, give drugs to increase insulin receptor sensitivity or even give insulin directly in an attempt to regulate the blood glucose levels of these patients or clients. This is a catch-22 because while the insulin receptors on muscle cells may be resistant and require increased amounts of the hormone to affect glucose uptake, other tissues and organs retain their sensitivity to insulin and prolonged exposure to high levels of the hormone invariably will lead to complications. Insulin stimulates sodium retention by the kidney, thus contributing to water retention and hypertension. At Ideal Protein, we believe that the Metabolic Syndrome is a problem caused by food (high carbohydrate intake, i. When we put patients or clients on a ketogenic diet we immediately decrease insulin levels and many symptoms quickly improve. This has been confirmed by hundreds of before-and-after fasting insulin levels in patients or clients seen in clinics that have adopted our weight loss protocol. In addition, there is ongoing support from our corporate medical staff and continual in-house service provided free of charge by our field representatives. Ketosis simply means the body is using fat as an energy source and is transforming fatty acids into ketonic bodies. This is a normal metabolic function like glycogenolysis, gluconeogenesis, or glycolysis and is totally safe as opposed to the pathological condition of ketoacidosis. Unfortunately, many nutritional consultants will say a diet that greatly restricts carbohydrate intake is dangerous as can deprive the glucose dependent tissues of their sole energy source and can also lead to severe hypoglycemia. If a deprivation of glucose occurs, the body will begin to break down its fat reserves (triglycerides). Simultaneously, some muscle is broken down and the amino acid alanine is converted into glucose in the liver via another gluconeogenic process the alanine glucose cycle. The kidneys use yet another pathway and convert the amino acid glutamine into even more glucose (incidentally this process also helps maintain proper acid/base balance thus preventing ketoacidosis. Hypoglycemia therefore occurs, not because of a lack of glucose (no lack of glucose occurs) but rather because of an overproduction of insulin following the ingestion of a high glycemic carbohydrate. Hypoglycemia should be more properly termed reactive hypoglycemia and this condition will almost always resolve completely within two weeks of the protocol. Finally remember, our interventional phase is not a lifestyle, there is a beginning and an end. Think of it as a bridge to a well-balanced diet in which healthy, complex carbohydrates are essential. Preoperative weight loss with a very-low energy diet: Quantitation of changes in liver and abdominal fat by serial imaging. The Ideal Protein Weight Loss Protocol is medically designed to promote weight loss while sparing muscle mass. Tran focused his career and research on nutrition with a particular emphasis on the treatment of obesity and obesity related issues. The Ideal Protein Weight Loss Protocol is a 4-Phase protocol that encourages pancreas and blood sugar levels stabilization while burning fat and maintaining muscle and other lean tissue. Our products are only available through trained and certified health professionals. Each Ideal Protein establishment has one or more experts to guide the patient or client through the program. This valuable process serves to educate and encourage the patients or clients with a consistent protocol that is scientifically proven and deemed by most as easy to execute and maintain. Increased consumption of more energy-dense, nutrient-poor foods with high levels of sugar and saturated fats, combined with reduced physical activity and stress, all have contributed to where we are today, a state that the World Health Organization has no qualms labeling as an obesity epidemic. To qualify as part of this epidemic that is steamrolling North America, adults or children need only suffer from two of the four components of the metabolic syndrome: 1. A diet grossly disproportionate in its share of saturated fats and sugars, such as in breads, cereals, muffins, cakes, pastries, pasta, pizza, rice, corn very much like the North American diet causes the pancreas to produce an overabundance of insulin, which stays in the system and puts the blood sugar level in a negative balance. Even worse, it locks the fat in the fat cell, preventing it to be used as a source of energy. The body employs energy from three reserves: glycogen (carbohydrate), protein and fats. Until 100% of the weight loss goal is achieved, we restrict carbohydrates (simple and complex). Remember, the first source of energy is derived from glycogen (carbohydrate) reserves. The main principle is to deplete the glycogen (carbohydrate) reserves completely in order to compel the body to turn to its fat reserve to burn calories. How do we encourage the body to burn its fat reserves and encourage its muscle mass maintenance, if both are depleted simultaneously First, by providing the body with foods that have a high protein value, complete with 8 essential amino acids, 97% absorbable, which make them biologically complete proteins. Second, by supplementing with nutrient-rich supplements such as Natura Multi-Vita, Natura Calcium and Magnesium, Omega-3 Plus and Potassium, key ingredients in muscle building and electrolytes to replace those normally found in foods while restricted on the Ideal Protein Weight Loss Protocol. Protocol Support Material 2 Revised March 22, 2017 the Ideal Protein Food Selection the centerpiece of our weight loss protocol is our gourmet protein based foods, which the patient or client will consume during the weight loss phases of the program. These are high biological value proteins and employ six different proteins, varying from products to products: whey isolates, soy isolates, whole milk protein, pea protein, albumin, and hydrolyzed collagen. This gives the client many options and is designed so people with sensitivities to dairy, soy or vegetarians may participate in the program. They are delicious, practical, satisfying and are available in an array of textures and flavors.
M em ory T Cell Dynam ics in the Lung during Inuenza Virus Infection Angela Pizzolla and Linda M medicine 95a order zyprexa with amex. It causes signicant animal reservoirs spreads rapidly worldwide treatment yeast uti generic zyprexa 5mg without a prescription, having a devas morbidity and mortality symptoms 5dpiui generic zyprexa 10 mg otc, particularly among immuno tating impact on global health medicine on airplane discount zyprexa 10 mg free shipping. This is dicates that inuenza-specic T cells resident along the because T cells recognize internal and more conserved parts respiratory tract are highly effective at providing potent of the inuenza virus that are far less prone to mutation and rapid protection against this inhaled pathogen medicine youth lyrics purchase zyprexa without a prescription. Experiments in animal models clearly highlight the these T cells recognize fragments of the virus that are importance of T cell immunity in the protection against highly conserved and less prone to mutation treatment hyponatremia best order zyprexa, they have inuenza virus. In addition to the loss of life, both seasonal circulating inuenza strains as well as newly annual inuenza outbreaks are a major burden on global emerging pandemic viruses. Dening parameters that promote economies because of the direct cost of healthcare as well as inuenza-specic lung-resident memory T cell formation and lost productivity due to illness. However, as these glycoproteins mu will discuss factors inuencing their induction, function, tate frequently, it is necessary to reformulate and administer and persistence. In addition, we will review exciting new vaccines annually to maintain protective immunity (2). Wakim, Department of Copyright O2019 by the American Association of Immunologists, Inc. This secondary antigenic interaction is directed transition into a long-lived memory cell. Trm located along an infection heavily inuences effector T cell survival and the respiratory tract are indispensable for optimal cross memory T cell development (70). Trm represent a self-sustaining, nonmigratory virus infection impacts the selection of different specicities of population of memory T cells that are deposited within T cells into the Trm pool (15, 19, 99). Trm transcriptional prole is aggressive decay with an estimated t1/2 of just 2 wk (97). Induction of partial specic het erotypic immunity in mice by a single infection with inuenza a virus. Generation of both cross-reactive and virus-specic T-cell populations after immunization with T cell response but also will need to ensure the memory T cell serologically distinct inuenza A viruses. Anti-inuenza virus cytotoxic T lymphocytes recognize the three viral polymerases and a non to develop vaccination regimes that specically evoke this structural protein: responsiveness to individual viral antigens is major histocom memory T cell population. Identication of viral respiratory tract Trm requires local cognate Ag recognition, molecules recognized by inuenza-specic human cytotoxic T lymphocytes. Functional analysis of inuenza-specic must deliver the vaccine Ag intranasally into the airways. T cells specic for internal viral proteins provide Studies in animal models have shown that intranasal immu cognate help for B cell responses to hemagglutinin. Do L3T4+ T cells act as effector cells in protection against inuenza virus infection. Effector mechanisms and evoke lung Trm that are highly protective against inuenza their longevity. Lung niches for the generation and maintenance of tissue resident memory T cells. Vaccine-generated lung tissue tion against a wide breadth of inuenza viruses, including resident memory T cells provide heterosubtypic protection to inuenza infection. Shortman, gene regulatory module functions as a read-write integrator to dynamically coor F. Genome-wide screening of human T-cell epitopes in inuenza target cell interaction: manifestation of a dual activation threshold. T cell lung homing and promote lung immunity through the chemokine receptor Cytokine Growth Factor Rev. Schumacher, and signals support sustained surveillance of the lungs by pathogen-specic cytotoxic J. Early establishment of diverse T cell receptor proles for mediates adhesion of activated intraepithelial lymphocytes to collagen. Nature 440: T cells persist in the lungs following recovery from respiratory virus infections. A novel peptide-based pan-inuenza A T cells in respiratory tract following inuenza infection. Truscott, inuenza virus induced by intranasal carbomer-lecithin-adjuvanted non-replicating G. Holst, response that correlates with reduction in symptomatology and virus shedding in a A. Combined local and systemic im randomized phase ib live-virus challenge in humans. In this review, reassortment, through which a virus can acquire a novel ge we examine the innate and adaptive immune responses notype by deriving entire gene segments from two different to avian inuenza viruses and their role in disease parent viruses that coinfect a cell. The outbreak of human infections was lated in various combinations from waterfowl and shorebirds. However, the precursor viruses con spill over into other hosts, including other avian species, such tinued to circulate in wild birds, and the viruses re-emerged in as chickens or turkeys, or mammals, in which they can cause humans in 2004 and continue to cause sporadic human cases a range of consequences, from asymptomatic infection to (6). The World Health Copyright O2019 by the American Association of Immunologists, Inc. Still others, including studied ex vivo in human monocyte-derived macrophages and H7N7, H7N3, H7N2, H7N4, and H9N2 viruses, have caused primary human airway cells (reviewed in Ref. H5N1 infection of primary endothelial cells (33, milder illnesses have been reported (22, 23). As was seen with H5N1 proinammatory cytokines and chemokines that have been infections, H7N9 infection in humans causes rapidly progressive reported in H5N1-infected patients, and is believed to play a pneumonia, with leukopenia and lymphopenia and substantially role in disease pathogenesis. The early host increased serum cytokine and chemokine concentrations in fatal response to H5N1 virus infection was investigated in cyn cases (25). In a subsequent case series of genes, as well as genes important in the acute phase re 256 patients, 65. However, the intense host required mechanical ventilation or extracorporeal membrane response was unable to control the rapidly progressing in oxygenation, revealed that cell cycle and neutrophil-related fection in this model (39). Infection with novel avian inuenza viruses triggers innate and adaptive immune responses. Overactivation of the innate immune system results in the production of high levels of inammatory cytokines by infected epithelial cells and innate immune cells. Ferrets are the preferred model for studying or stem are some of the key changes that were made in the inuenza disease and transmission, but there are limited assays (reviewed in Ref. Furthermore, H5N1 eggs would provide 10 to 100-fold more doses per egg than infections in humans resulted in the local activation of the inactivated subunit vaccine. Under a collaborative research oxidative stress machinery and oxidized phospholipid for and development agreement with MedImmune, we generated mation in the lungs (71). However, it quickly became clear that backbone were safe and well tolerated, but primary vaccination H5 and H7 vaccines did not induce nearly as robust an Ab did not elicit an immune response that was detectable by response as seasonal inuenza vaccines (reviewed in Ref. The Ab titer declined rapidly (within recalled with a dose of inactivated subunit vaccine. Inactivated H7N7 and sufficiently well to confer protection, it is difficult to envision H7N9 subunit vaccines were also poorly immunogenic when a scenario to prove it. In 2009, the H1N1 pandemic was caused There is an enormous genetic and antigenic diversity among by a virus that was not recognized to pose a pandemic threat. A completely novel approach to achieve peak viral replication occurs within 2 d of infection. These data are subtypes and were highly effective in protecting experimental supported by studies in animal models. Origin of the pandemic 1957 H2 inuenza A virus and the persistence of its nous Australians and Alaskans, because of ethnic differences in possible progenitors in the avian reservoir. Shortridge, Transmission of H7N7 avian inuenza A virus to human beings during a large S. Induction of proinammatory cyto outbreak in commercial poultry farms in the Netherlands. Qiu, early block in the replication cycle to promote productive replication in macro K. Epidemiology of avian inuenza A H7N9 virus in Fatal outcome of human inuenza A (H5N1) is associated with high viral load and human beings across ve epidemics in mainland China, 2013-17: an epidemio hypercytokinemia. Preliminary epidemiology of human infections with highly Early and sustained innate immune response denes pathology and death in pathogenic avian inuenza A(H7N9) virus, China, 2017. Clinical and epidemiological characteristics of a fatal case of in patients naturally infected by H5N1 virus. Lancet 354: natural infection, live cold-adapted vaccine, and inactivated vaccine. Global epidemiology of avian inuenza A against H5N1 in mice and are present in unexposed humans. Mahmood, features and rapid viral diagnosis of human disease associated with avian inuenza G. Nguyen-Van-Tam, et al; Flu virus from wet market poultry: clinical analysis and characterisation of viral ge Watch Group. Tong, booster vaccination: an open non-randomised extension of a double-blind rand A. Geelhoed-Mieras, diversity and affinity of antibody-mediated immune response to pandemic inu M. Liebner, Correlates of immune protection induced by live, attenuated, cold-adapted, tri R. Development of live a polymerase protein of an H5N1 inuenza virus is associated with systemic in attenuated inuenza vaccines against pandemic inuenza strains. Pandemic preparedness with live at of lymphocytes and diminished cytokine production in mice infected with a highly tenuated inuenza vaccines based on A/Leningrad/134/17/57 master donor virus. Schappell, pression analysis of host innate immune responses during Lethal H5N1 infection T. Dilorenzo, Transforming growth factor-b: activation by neuraminidase and role in highly J. Chen, virus infection in macaques is associated with early dysregulation of inammatory C. DiLorenzo, cation of oxidative stress and Toll-like receptor 4 signaling as a key pathway of G. A live attenuated H7N3 inuenza virus vaccine is well tolerated and immunogenic 72. An Safety and immunogenicity of an inactivated subvirion inuenza A (H5N1) vac open label phase I trial of a live attenuated H6N1 inuenza virus vaccine in healthy cine. King, Evaluation of the safety and immunogenicity of a booster (third) dose of inacti B. Intranasal live inuenza vaccine priming elicits localized B cell responses in 76. Mayall, nogenicity of a subvirion inactivated inuenza A/H5N1 vaccine with or without J. Wood, H5N1 inuenza: a randomised, double-blind, placebo-controlled, phase 1 study. Avian inuenza h6 viruses productively infect vaccine: a randomised controlled trial. Koudstaal, Evaluation of replication and pathogenicity of avian inuenza a H7 subtype viruses M. Schultz-Cherry, by human cytotoxic T-lymphocyte populations directed to human inuenza A C. Zheng, of heterosubtypic protection in ferrets and pigs induced by a single-cycle inuenza J. Fernandez delivery of a candidate universal inuenza vaccine reduces viral load in pigs Rodriguez, F. The vaccine is ad Centers for Disease Control andPreventionreportedover ministered i. How the severity of this inuenza season highlights the importance of ever, these viruses have been engineered to grow at or below measures to control and even prevent inuenza virus infections. Because they are attenuated live viruses, they is through vaccination. It requires continually updating the vaccine to Health Organization advisory group of experts meet biannually keep up with viral evolution.
References
- Caramori G, Adcock IM, Casolari P, et al. Unbalanced oxidant-induced DNA damage and repair in COPD: a link towards lung cancer. Thorax 2011; 66: 521-527.
- Li H, Schwartz NB, Vertel BM: cDNA cloning of chick cartilage chondroitin sulfate (aggrecan) core protein and identification of a stop codon in the aggrecan gene associated with the chondrodystrophy, nanomelia, J Biol Chem 268(31):23504-23511, 1993.
- Wu B, Liu H, Huang J, et al. Pulmonary cryptococcosis in non-AIDS patients. Clin Invest Med 2009; 32: E70-E77.
- Kelly RA, Han X: Nitrovasodilators have (small) direct effects on cardiac contractility: Is this important? Circulation 96:2493, 1997.
- Wielopolski PA, van Geuns RJ, et al. Breath - hold coronary MR angiography with volume - targeted imaging. Radiology 1998; 209:209.
- Williams, D.M., E.S. Anderson, and R.A. Winett, A review of the outcome expectancy construct in physical activity research. Ann. Behav. Med., 2005.
- Duckett JW: Hypospadias techniquesoupdate 1984.