
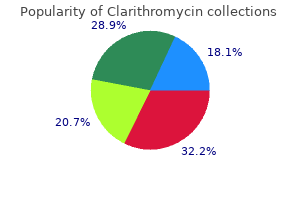
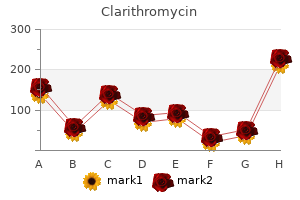
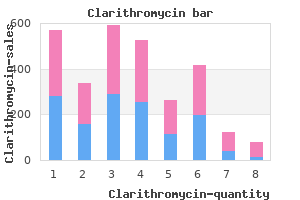
Clarithromycin

Allan I. Basbaum PhD
- Professor and Chair, Department of Anatomy and W.M. Keck Foundation Center for integrative Neuroscience, University of California, San Francisco

https://bms.ucsf.edu/faculty/allan-basbaum-phd
Docetaxel is showing impressive benefits gastritis diet ����� safe 250mg clarithromycin, with fewer side effects gastritis diet ������� order clarithromycin 500mg online, in these conditions chronic gastritis flatulence discount clarithromycin online. They bind reversibly to the Itubulin subunit severe erosive gastritis diet order genuine clarithromycin line, but unlike the vinca alkaloids chronic gastritis food to avoid cheap clarithromycin express, they promote polymerization and stabilization of the polymer rather than disassembly ure 39 gastritis diet xp order 500 mg clarithromycin with amex. Thus, they shift the depolymerizationpolymerization process to accumulation of microtubules. The overly stable microtubules formed are nonfunctional, and chromosome desegregation does not occur. Resistance: Like the vinca alkaloids, resistance has been associated with the presence of amplified Pglycoprotein or a mutation in the tubulin structure. Hepatic metabolism by the cytochrome P450 system and biliary excretion are responsible for their elimination into the stool. Thus, dose modification is not required in patients with renal impairment, but doses should be reduced in patients with hepatic dysfunction. Adverse effects: the doselimiting toxicity of paclitaxel and docetaxel is neutropenia. A transient, asymptomatic bradycardia is sometimes observed with paclitaxel, and fluid retention is seen with docetaxel. Because of serious hypersensitivity reactions (including dyspnea, urticaria, and hypotension), a patient who is to be treated with paclitaxel is premedicated with dexamethasone and diphenhydramine as well as with an H2 blocker. Hormone treatment of responsive tumors usually is only palliative, except in the case of the cytotoxic effect of glucocorticoids at higher doses (for example, prednisone) on lymphomas. Removal of hormonal stimuli from hormonedependent tumors can be accomplished by surgery (for example, in the case of orchiectomy for patients with advanced prostate cancer) or by drugs (for example, in breast cancer, for which treatment with the antiestrogen tamoxifen is used to prevent estrogen stimulation of breast cancer cells). For a steroid hormone to influence a cell, that cell must have intracellular (cytosolic) receptors that are specific for that hormone ure 39. Mechanism of action: Prednisone itself is inactive and must first be reduced to prednisolone by 11Ihydroxysteroid dehydrogenase. Resistance: Resistance is associated with an absence of the receptor protein or a mutation that lowers receptor affinity for the hormone. However, in some resistant cells, a receptorhormone complex is formed, although a stage of gene expression is apparently affected. The latter is glucuronidated and excreted into the urine along with the parent compound. Adverse effects: Prednisone has many of the adverse effects associated with glucocorticoids. It can predispose to infection (due to its immunosuppressant action) and to ulcers and pancreatitis. Other effects include hyperglycemia, cataract formation, glaucoma, osteoporosis, and change in mood (euphoria or psychosis). It also finds use prophylactically in reducing breast cancer occurrence in women who are at high risk. However, because of possible effects stimulating premalignant lesions due to its estrogenic properties, tamoxifen is presently approved only for 5 years of use. Mechanism of action: Tamoxifen binds to the estrogen receptor, but the complex is transcriptionally not productive. The result is a depletion (downregulation) of estrogen receptors, and the growthpromoting effects of the P. Resistance: Resistance is associated with a decreased affinity for the receptor or the presence of a dysfunctional receptor. Some metabolites possess antagonist activity, whereas others have agonist activity. Unchanged drug and its metabolites are excreted predominantly through the bile into the feces ure 39. Adverse effects: Side effects caused by tamoxifen are similar to the effects of natural estrogen, including hot flashes, nausea, vomiting, skin rash, vaginal bleeding, and discharge (due to some slight estrogenic activity of the drug and some of its metabolites). Arom atase inhibitors the aromatase reaction is responsible for the extraadrenal synthesis of estrogen from androstenedione, which takes place in liver, fat, muscle, skin, and breast tissue, including breast malignancies. Peripheral aromatization is an important source of estrogen in postmenopausal women. Aminoglutethimide was shown to inhibit both the adrenal synthesis of pregnenolone (a precursor of estrogen) from cholesterol as well as the extraadrenal synthesis. Because the drug also inhibits hydrocortisone synthesis, which evokes a compensatory rise in adrenocorticotropic hormone secretion sufficient to overwhelm the blockade of the adrenal, the drug is usually taken with hydrocortisone. Due to its nonselective properties and unfavorable side effects, as well as the need to concomitantly administer hydrocortisone (cortisol), newer aromatase inhibitors (described below) have been developed. They have gained favor in the treatment of breast cancer because 1) they are more potent (they inhibit aromatization by greater than 96 percent, compared to less than 90 percent with aminoglutethimide), 2) they are more selective than aminoglutethimide, 3) they do not need to be supplemented with hydrocortisone, 4) they do not predispose to endometrial cancer, and 5) they are devoid of the androgenic side effects that occur with the steroidal P. Although anastrozole and letrozole are considered to be secondline therapy after tamoxifen for hormonedependent breast cancer in the United States, they have become firstline drugs in other countries for the treatment of breast cancer in postmenopausal women. They are orally active and cause almost a total suppression of estrogen synthesis. Because the metabolites are excreted into the urine, doses of the drug must be adjusted in patients with renal failure. Response to leuprolide in prostatic cancer is equivalent to that of orchiectomy (surgical removal of one or both testes), with regression of tumor and relief of bone pain. These drugs have some benefit in premenopausal women with advanced breast cancer and have largely replaced estrogens in therapy for prostate cancer. Leuprolide is available 1) as a sustainedrelease preparation, 2) subcutaneous, or 3) as a depot intramuscular injection to treat metastatic carcinoma of the prostate. The adverse effects of these drugs, including impotence, hot flashes, and tumor flare, are minimal compared to those experienced with estrogen treatment. Estrogens Estrogens, such as ethinyl estradiol or diethylstilbestrol, had been used in the treatment of prostatic cancer. Estrogen treatment can cause serious complications, such as thromboemboli, myocardial infarction, strokes, and hypercalcemia. They compete with the natural hormone for binding to the androgen receptor and prevent its translocation into the nucleus (see ure 39. Flutamide is metabolized to an active hydroxy derivative that binds to the androgen receptor. Therefore, flutamide is always administered in combination with leuprolide or goserelin which can desensitize the hypothalamuspituitary axis. Monoclonal Antibodies Monoclonal antibodies have become an active area of drug development for anticancer therapy and other nonneoplastic diseases, because they are directed at specific targets and often have fewer adverse effects. They are created from B lymphocytes (from immunized mice or hamsters) fused with a fiimmortala Blymphocyte tumor cells. The resulting hybrid cells can be individually cloned, and each clone will produce antibodies directed against a single antigen type. Recombinant technology has led to the creation of a fihumanizeda antibodies that overcome the immunologic problems previously observed following administration of mouse (murine) antibodies. Currently, several monoclonal antibodies are available in the United States for the treatment of cancer. The drug, usually administered with paclitaxel, can cause regression of breast cancer and metastases in a small percentage of these individuals. They have been implicated in the development of many neoplasms by an unknown mechanism. Mechanism of action: How the antibody causes its anticancer effect remains to be elucidated. Efforts are being directed toward identifying those patients with tumors that are sensitive to the drug. Adverse effects: the most serious toxicity associated with the use of trastuzumab is congestive heart failure. Extreme caution should be exercised when giving the drugs to patients with preexisting cardiac dysfunction. Other adverse effects include infusionrelated fever and chills, headache, dizziness, nausea, vomiting, abdominal pain, and back pain, but these effects are well tolerated. Rituximab has proven to be effective in the treatment of posttransplant lymphoma and in chronic lymphocytic leukemia. Pretreatment with diphenhydramine, acetaminophen, and bronchodilators can ameliorate these problems. Tumor lysis syndrome has been reported within 24 hours of the first dose of rituximab. Leukopenia, thrombocytopenia, and neutropenia have been reported in less than 10 percent of patients. It attaches to and stops vascular endothelial growth factor from stimulating the formation of new blood vessels. Without new blood vessels, tumors do not receive oxygen and essential nutrients necessary for growth and proliferation. The most common adverse effects of this treatment are hypertension, stomatitis, and diarrhea. Less common are bleeding in the intestines, protein in the urine, and heart failure. Among the rare serious side effects are bowel perforation, opening of healed wounds, and stroke. It is believed to exert its antineoplastic effect by targeting the epidermal growth factor receptor on the surface of cancer cells and interfering with their growth. Cetuximab has caused difficulty breathing and low blood pressure during the first treatment, and interstitial lung disease has been reported. The mechanisms of action of the two drugs are similar, but their potency, pharmacokinetics, patterns of distribution, and doselimiting toxicities differ significantly. Cisplatin has synergistic cytotoxicity with radiation and other chemotherapeutic agents. Carboplatin is employed when patients cannot be vigorously hydrated, as is required for cisplatin treatment, or if they suffer from kidney dysfunction or are prone to neuro or ototoxicity. Mechanism of action: the mechanism of action for this class of drugs is similar to that of the alkylating agents. In the highchloride milieu of the plasma, cisplatin persists as the neutral species, which enters the cell and loses its chlorides in the lowchloride milieu. Similarly, the chemical moieties that replace the chlorides in the carboplatin structure are removed hydrolytically to form the active drug. Cytotoxicity can occur at any stage of the cell cycle, but cells are most vulnerable to the actions of these drugs in the G1 and S phases. They can also be given intraperitoneally for ovarian cancer and intraarterially to perfuse other organs. More than 90 percent of cisplatin is covalently bound to plasma proteins, but the binding of carboplatin to plasma proteins is very low. Adverse effects: Severe, persistent vomiting occurs for at least 1 hour after administration of cisplatin and may continue for as long as 5 days. The major limiting toxicity is doserelated nephrotoxicity, involving the distal convoluted tubule and collecting ducts. Patients concomitantly receiving aminoglycosides are at greater risk for nephrotoxicity and ototoxicity. Unlike cisplatin, carboplatin causes only mild nausea and vomiting, and it is not nephro, neuro, or ototoxic. They have a complicated multiring structure containing a lactone ring that is essential for activity. Topotecan is employed in metastatic ovarian cancer when primary therapy has failed and also in the treatment of smallcell lung cancer. Therefore, the dose may have to be modified in patients with impaired kidney function. Frequent peripheral blood counts should be performed on patients taking this drug. Nonhematologic effects include diarrhea, nausea, vomiting, alopecia, and headache. Myelosuppression is also seen with irinotecan, and delayed diarrhea may be severe and require treatment with loperamide. Resistance to topoisomerase inhibitors is conferred either by presence of the multidrugresistant Pglycoprotein or by mutation of the enzyme. Etoposide finds its major clinical use in the treatment of oatcell carcinoma of the lung and in combination with bleomycin and cisplatin for testicular carcinoma. Teniposide is used as a secondline agent in the treatment of acute lymphocytic leukemia. Despite this, teniposide has shown effectiveness against gliomas and neuroblastomas. Metabolites are converted to glucuronide and sulfate conjugates and are excreted in the urine. Drugs that induce the cytochrome P450 system lead to an acceleration of teniposide metabolism. Doselimiting myelosuppression (primarily leukopenia) is the major toxicity for both drugs. The ability of imatinib to occupy the a fikinase pocketa prevents the phosphorylation of tyrosine on the substrate molecule and, hence, inhibits subsequent steps that lead to cell proliferation. It undergoes metabolism by the cytochrome P450 system to several compounds, of which the Ndemethyl derivative is active.
Syndromes
- Reaction to snake or insect venom
- The bottom number indicates the distance at which a person with normal eyesight could read the same line you correctly read.
- Amount swallowed
- Bulging eyeball, usually on one side of face
- Breathing - slow
- Hematoma (blood accumulating under the skin)
- Torn labrum
- Coronary artery disease (CAD)
- Meningitis
- Ankylosing spondylitis
Smith was newly diagnosed by his primary care physician with type 2 diabetes with hyperglycemia (E11 chronic superficial gastritis definition clarithromycin 250 mg discount. Smith also has a documented history of chronic prepyloric gastritis definition purchase 500mg clarithromycin mastercard, systolic (congestive) heart failure (I50 gastritis symptoms foods avoid order cheap clarithromycin on-line. Jones was discharged from the hospital status post colectomy with colostomy placement for colon cancer gastritis diet book order generic clarithromycin from india. Disclaimer: All scenarios are for illustrative purposes and assumption is that these beneficiaries meet all criteria for home health services gastritis journal articles order cheap clarithromycin line. Gray requires a home health aide three times a week to assist with bathing and dressing chronic gastritis support group buy clarithromycin visa. Only the final home health claim would be adjusted to reflect the institutional admission. Medicare policy changes frequently so links to the source documents have been provided within the document for your reference this presentation was prepared as a service to the public and is not intended to grant rights or impose obligations. This presentation may contain references or links to statutes, regulations, or other policy materials. We encourage readers to review the specific statutes, regulations, and other interpretive materials for a full and accurate statement of their contents 82. The primary outcome Institute of Health Innovation, Macquarie University, Sydney (V. Secondary outcomes in at the Physiotherapy Department, Calvary cluded cellulitisrelated hospital admission and qualityoflife assessments. A total of 3 participants (7%) in the com pression group and 6 (14%) in the control group were hospitalized for cellulitis (hazard ratio, 0. Compression Therapy to Prevent Cellulitis of the Leg ellulitis is a common bacterial in Methods fection of the skin and subcutaneous tis Trial Design and Oversight Csue that occurs mostly in the legs and is associated with health care costs and adverse1 Participants were randomly assigned in a 1:1 health outcomes. Recurrence of cellulitis is2 ratio to receive either compression therapy plus common: up to 47% of patients have a recurrent education regarding prevention of cellulitis (com episode within 3 years. Partici progressively once the antibiotic agent is discon pants in the control group crossed over to the tinued. A Cochrane review of interventions to4 compression group when they had an episode of prevent cellulitis identified six studies investi cellulitis. Assessors and participants were aware gating prophylactic antibiotics, but no random of the trialgroup assignments. The proto nonantibiotic treatments to prevent cellulitis has col (available with the full text of this article at not been well studied. Participants for 3 months or longer and has various and of provided written informed consent before the ten mixed causes. The authors designed and implemented may be increased capillary filtration or failure of the trial and collected and analyzed the data. The lymphatic drainage, 7, 8 which results from condi first author wrote the first draft of the manu tions such as lymphedema, venous hypertension, script, and all authors contributed to subsequent immobility, obesity, and heart failure. The authors vouch for the accuracy and edema is a risk factor for cellulitis of the leg and completeness of the data and for the adherence for recurrent cellulitis. Haddenham Health Compression therapy has been used to reduce care manufactured and provided the compres and control chronic edema. This treatment in sion garments but had no involvement in the volves the daily wearing of compression garments design, conduct, analysis, or reporting of the such as stockings, with or without a short period trial and did not have access to the trial data. Compres Participants sion garments and bandages exert the greatest Participants were recruited at one of two primary degree of compression at the ankle and gradu public hospitals or were referred by general prac ally apply less pressure proximally along the limb. Patients were By exerting this type of graduated pressure on eligible to participate if they had a history of two the leg, compression therapy reduces the forma or more episodes of cellulitis in the same leg in tion and accumulation of interstitial fluid and the 2 years before referral to the trial and had shifts fluid proximally, away from the lower leg. Full inclusion sion therapy to prevent recurrent cellulitis in pa and exclusion criteria are provided in the proto tients with chronic edema of the leg, and com col. The presence of edema was confirmed by pression therapy is widely used by clinicians2, 3, 13, 14; means of interview and physical examination by however, there are limited data from trials to specialist lymphedema physiotherapists. We conducted a random were excluded from the trial if they were young ized, controlled, singlecenter trial to determine er than 18 years of age, were already wearing whether compression therapy would prevent the effective compression garments 5 or more days recurrence of cellulitis of the leg in adults with per week, were receiving endoflife care, had a chronic edema of the leg. The new england journal of medicine wound or a wound requiring specialist treatment, lulitis recurrence and associated hospital admis or if compression therapy was contraindicated. Participants assigned to the compression class 1 garments (providing 18 to 21 mm Hg of group were instructed to wear compression gar pressure) were excluded if a lymphedema thera ments throughout the day and were provided pist determined that this lower amount of pres information on use, safety, cleanliness, and ap sure was effective for the patient. Two free sets of compression garments were provided to Interventions and Assessments participants in the compression group at the All assessments and interventions were performed beginning of the trial and to participants in the in the outpatient department of the hospital by control group when they crossed over to the com specialist lymphedema physiotherapists who were pression group. Baseline When appropriate, a short period (typically 3 to measures, including demographic characteristics, 5 days) of therapistapplied compression bandag leg volume, and quality of life, were recorded ing to minimize edema was provided immedi before randomization. Cellulitis was diagnosed ately before the compression garments were fit by general medical practitioners or by hospital ted. The majority of prescribed the trial; the diagnosis was confirmed by trial compression garments were kneehigh compres assessors. Trial assessors verified the dates of sion stockings that included the foot, with or recurrence and hospitalization with the use of without the toes. The report episodes of cellulitis at the time that they number of appointments required to provide occurred. In addition, participants were inter compression therapy was not prespecified and viewed at the 6month followup appointments varied according to the individual needs of the to determine whether there had been unreported participants. If a recurrence was re the prescribed garment type and compression ported between scheduled followup appoint class were determined on the basis of edema ments, participants were seen for an additional severity, leg shape, skin condition, and the ease appointment with a lymphedema therapist to of application and removal by the participants or record outcome measures (date of cellulitis diag their caregivers. If chronic edema was present in nosis and associated hospitalization); participants both legs, compression therapy was provided for in the control group commenced crossover to both legs. An episode was recommended after 6 to 12 months of wear, of cellulitis was recorded only if it occurred in a with no restrictions on the brand used. Qualityoflife date of crossover was defined as the day that measures, leg volume, adherence to wearing gar compression garments were initially fitted. Par ments in the compression group, and adverse ticipation in the trial was terminated in the case events were assessed at the 6month appoint of death, withdrawal of consent, or development ments. If participants could not attend their of a wound or lymphorrhea for which manage scheduled appointments, assessment was per ment with compression therapy was advised and formed by means of telephone to check for cel was supported by evidence. Compression Therapy to Prevent Cellulitis of the Leg measures were obtained for participants who of cellulitis in the compression group than in the were withdrawn from the trial. On the basis of these assumptions, we hospital admission, change in leg volume, and planned to recruit 162 participants (see the Sup qualityoflife measures. Randomization was strat sured with the use of a perometer (an optoelec ified according to prophylactic antibiotic use, tronic imaging device). The perometer was identical envelopes were used to ensure conceal calibrated to a standardized object every 2 weeks ment of trialgroup assignments. If the trial continued until 45 encompasses four domains (symptoms, appear episodes of cellulitis occurred, the final analysis ance, function, and mood), each scored at four would use a logrank test with a onesided sig levels (not at all, a little, quite a bit, or a lot; com nificance level of 0. Therefore, no data on outcomes for partici [best imaginable health state]) and a descriptive pants who crossed over to the compression group system that assesses five dimensions of quality were included in the primary analysis. For the of life (mobility, personal care, usual activities, secondary outcomes of leg volume and quality of pain and discomfort, and anxiety and depression) life, data for each participant in the control group at three levels (no problems, some problems, or were collected until crossover occurred, and data extreme problems; total scores for the descrip for participants in the compression group were tive system range from 5 to 15, with lower scores collected until the last participant in the control indicating better quality of life). The logrank test was used to pants during the 6month assessments with test for betweengroup differences. The propor Assuming that recurrence of cellulitis at 3 years tionalhazards assumption was assessed with would occur in 47% of participants in the con the use of correlation of scaled Schoenfeld re trol group (on the basis of previous reports3, 4) siduals and transformed survival time (cox. The new england journal of medicine Mixedeffects linear models were used to as sess betweengroup differences in the change in 183 Patients were referred for screening leg volume and quality of life over time, with group and time as fixed effects and participant 32 Were not assessed identification number as the random effect. The 17 Did not attend initial assessment 3 Died two components of each qualityoflife scale were 12 Were not recruited analyzed separately. There was no plan for adjustment for multiple comparisons in the 151 Patients were assessed for eligibility analyses of secondary outcomes, and the widths of confidence intervals were not adjusted for 67 Were excluded multiplicity; therefore, no clinical conclusions 25 Did not have recurrent leg can be made from these data. The statistical cellulitis 11 Did not have chronic edema analysis plan is available with the protocol. All 14 Were already wearing effective analyses were performed with the use of R soft compression garments 21 2 Were in clinically unstable ware, version 3. In September 2018, after nine events of 84 Underwent randomization cellulitis had occurred in 67 participants, lymph edema therapists who were aware of the trial group assignments noted that there may have been a large betweengroup difference in recur rence. This potential difference between groups 41 Were assigned to the compres 43 Were assigned to the control was brought to the attention of the human re sion group group 39 Did not receive prophylactic 41 Did not receive prophylactic search ethics committees overseeing the trial. On March 26, 2019, 1 Died 1 Had wound requiring the data monitoring committee advised, on the 1 Had wound requiring intervention intervention 2 Were lost to followup basis of the post hoc stopping rule, that the 1 Moved trial should be stopped for efficacy and recruit 2 Were lost to followup ment should cease; the committee also recom mended that crossover should commence to 41 Were included in the intention 43 Were included in the intention provide participants in the control group with totreat analysis totreat analysis compression therapy. During the trial, 2 participants (5%) in each group were for Statistical Computing]). Data for 3 participants (7%) in tionalhazards assumption was not met, a post the compression group were censored because of hoc analysis of relative risk was performed. Data death (1 [2%]), occurrence of a wound (1 [2%]), for participants who were lost to followup were and relocation to a different state (1 [2%]). It is assumed that all participants had some degree of edema related to previous episodes of cellulitis. No other participants used prophylactic Baseline demographic characteristics were antibiotics before an episode of cellulitis during similar in the two groups (Table 1). Before provision of compression gar pants in each group were using prophylactic ments, 24 participants in the compression group antibiotics at the time of enrollment and contin received therapistapplied compression bandaging n engl j med 383;7 nejm. Compression stockings Hospital admission for cellulitis (a secondary were prescribed for all participants in the com outcome) occurred in 3 participants (7%) in the pression group, and a combination of compres compression group and in 6 (14%) in the control sion stockings and compression wraps were group (hazard ratio, 0. At the time of the interim analysis, the follow After 6 months, 1 participant (2%) in the com up time ranged from 0 to 511 days, with a median pression group and 5 (12%) in the control group of 186 days. The median less than that at baseline; among participants in followup was 209 days in the compression the control group, the mean leg volume had group and 77 days in the control group. Because data collection for leg volume score had decreased (reflecting a better quality and qualityoflife outcomes continued for par of life) by 0. No adverse outcomes were reported in participants who wore compression Discussion stockings or compression wraps. This singlecenter, nonblinded, randomized trial, Outcomes which was stopped early for efficacy, showed that At the time the trial was stopped, recurrence of compression therapy resulted in a lower inci cellulitis (the primary outcome) had occurred in dence of recurrent cellulitis than conservative 6 of 41 participants (15%) in the compression treatment in adults with chronic edema of the group and in 17 of 43 (40%) in the control group leg. Be analyses of hospitalization for cellulitis and of cause the proportionalhazards assumption was the change in leg volume from baseline were in not met, relative risk was calculated post hoc. Table adjustment for multiple comparisons of second S1 shows the results of the exploratory analysis ary outcomes precludes clinical conclusions from of the influence of factors that are typically as these data. Because the trial was stopped after square of the height in meters] fi40, tinea pedis the interim analysis, we were not able to report or toeweb intertrigo, fi3 episodes of cellulitis data on the 3year effect of compression therapy in either leg in the 2 years before enrollment, or on leg volume, as we had intended. The post hoc analysis of relative risk was performed because the proportionalhazards assumption was not met. The mean change (slope) was estimated with the use of mixedeffects linear models that included baseline data and all available followup data. We found that compression therapy re less likely to benefit from antibiotic prophylaxis duced cellulitis recurrence in the participants than other patients with cellulitis. All partici4 in our trial, who were at risk for failure of anti pants in our trial had one or more risk factors biotic prophylaxis. Future studies could explore the role of these mechanisms in cellulitis associated with 50 chronic edema of the leg. A potential source of bias in this trial is the fact that assessors and participants were aware 25 of the trialgroup assignments. Although the trial assessors, who were lymphedema therapists, had 0 no influence on making the diagnosis of celluli 0 60 120 180 240 300 tis, medical practitioners external to the trial Days since Enrollment who diagnosed cellulitis could have been influ No. Difficulty in applying and removing com lactic antibiotics can cause side effects, and the5 pression garments is often a barrier to adher bacterial species precipitating cellulitis is usually ence to compression therapy; however, in our unidentifiable, 23 which hinders targeted anti trial, 88% of the participants wore their gar biotic prophylaxis. This high adher use of compression therapy has been recom ence may have been the result of support from mended15 and has shown benefits in controlling experienced clinicians and may limit generaliz edema in patients with chronic edema of the ability of our findings to other settings in which leg20, 25, 26; in addition, its efficacy is not related to access to specialist lymphedema physiotherapists the causative bacterial species. Furthermore, aimed to reflect standard clinical practice, and compression therapy is the primary treatment we accepted the diagnosis of cellulitis as deter for lipodermatosclerosis, a condition that is often mined by medical practitioners. The point esti misdiagnosed as cellulitis31 and for which anti mates of differences in effect sizes between trial biotic treatment is ineffective. Larger and longer trials are We thank Robert Fleet for conducting the statistical analysis necessary in order to determine the effect of for the interim analysis and for participating as a member of compression therapy on the recurrence of cellu the independent data monitoring committee; Angie Fearon and Jeremy Witchalls for participating as members of the indepen litis, especially in settings without access to dent data monitoring committee; Ming Ling for assistance with specialized lymphedema services. Team (especially Gemma Arnold, MarieMichelle Coulombe, No potential conflict of interest relevant to this article was Emma May, Abby Benton, Caitlin Norris, Joshua Pogson, Alicia reported. Australian Commission on Safety and with shared care between primary and Compression therapy: a position document Quality in Health Care. A study of the advantages of elastic stock of the lower leg: a series with community 14. Br J Dermatol 2006;155:947 lulitis: risk factors, etiology, pathogenesis 15:2727. The management and treat prevention of cellulitis (erysipelas): results Riches K, Hilliam R.
The study showed an 85% success rate for the elimination of the alcoholic behavior of the men in the experimental group gastritis lower back pain buy clarithromycin 500mg free shipping. Not fully trusting this level of success gastritis empty stomach purchase 500 mg clarithromycin with visa, Menninger did its own private followup study 36 months later (Walters gastritis symptoms bad breath discount clarithromycin 250 mg, personal communi cation) gastritis diet en espanol discount 500 mg clarithromycin visa. They talked to each study subject gastritis symptoms in child purchase clarithromycin master card, their wives and their family members gastritis baby cheap generic clarithromycin uk, and found that the original outcomes were holding. According to these wellvalidated inventories most of the pathology of these personalities had normalized (Peniston and Kulkosky, 1990). In the original research the protocol involved fifteen 30minute sessions, typically performed twice a day, 5 days a week, on Veterans Administration Hospital inpatients. This visualization of the desired state also includes images of being already healed as an explicit way of instructing the unconscious to make it so, thus avoid ing ambiguities that may leave the door open to unintended interpretations. Moreover, inundating the unconscious with mental rehearsals of new conditions, and clear intentions of desired change, seems to effect healing and change both physiologically and psychologically (Green & Green, 1977; Achterberg, 1985; Simonton and Simonton, 1978). There is archaeological evidence suggesting that the techniques of the shaman using imagination for healing are at least 20, 000 years old, with vivid evidence of their antiquity in the cave paintings in the south of France. Asclepius, Aristotle, Galen, and Hippocrates, often regarded as the fathers of medicine, used imagery for diagnosis and therapy (Achterberg, 1985). That is, images may communicate with tissues and organs, even cells, to effect change (Simonton and Simonton, 1978;Achterberg, 1985; Rossi, 1986; Siegel, 1986). At our Institute we generally set the electrode at P4, near the area of the brain associated with boundaries of the self, and we set thresholds to assure at least 70% positive feedback with a warning signal for excessive delta (sleep wave) amplitudes. Regardless of the differences in placement, and varying ideas on feedback, results seem to be consistently positive in treatment of addictions and other symptomology. In the fight or fiight response, the body is alerted and blood fiow is increased to the major organs. To counter this state, as the peripheral circulation is increased with training, the body relaxes. In addition, rhythmic diaphragmatic breathing may be taught to still body functions and focus attention. Is it practical to take this protocol apart in its different aspects to find its power, or would this be reductionist thinking akin to examining the vocal cords to see how Nancy E. The power of this protocol seems to lie in its nonlinear interaction with many aspects of the brain/mind, and it may be of greater value to examine how these aspects contribute to an overall impact that creates a positive outcome for most patients treated. Empirical science, as we know it, seeks to understand reality from the point of view of the five senses. Toward the end of his life, Abraham Maslow, one of the major pioneers in humanistic psychology, called attention to possibilities beyond selfactualization in which the individual transcended the customary limits of identity and experi ence. Autopoiesis and the malleability of memory Life is not a static condition but a process. Autopoiesis sees the brain in a constant state of nonlinear development and redevelopment down to the dendrites themselves, which may extend into the synapse and retract with startling frequency, some extensions last ing only a few days (Trachtenberg et al. Thus we are as humans both being and becoming at once, and at all levels of existence. The earlier, linear view of the brain is based on the idea of specificity, which looks at the seeming invariants of the human brain as it develops. The emerging, dynamic (quantum) view of the brain focuses more on plasticity or the variations that develop as the brain adapts to environmental contingencies (Rose, 1994). We propose that neu rofeedback in all its forms rides on the back of neural plasticity and may be described more by developmental systems theory, of which autopoiesis is a specific expression, than by anatomy alone. Neuroplasticity tells us that the brain can be directed in that process of change by appropriate interventions. It is not that the effectiveness of neurofeedback is not provable; rather, that medical science has yet to incorporate systems theory in its approach. The malleability of memory is a behavioral manifestation of the plasticity of neural systems (Cozolino, 2002). Conversely, the plasticity of memory opens an avenue to the alteration of neural systems. That is, the intro duction of new information or new scenarios can modify affective reactions, and alter the nature of memories. In this state the patient not only has the opportunity to change the emotional content of the past, but can redirect his or her potential future from that new foundation. Statedependent memory and retrieval Malleability of memory depends in part on states of consciousness and arousal, known to psychology as the concept of statedependent memory and retrieval, or statecontext dependent learning and retrieval as Jon Cowan (1993) has expressed it. Rossi (1986) states that each time we access the statedependent memory, learning, and behavior pro cesses that encode a problem, we have an opportunity to reassociate and reorga nize, or reframe, that problem in a manner that resolves it. This reliving, releasing, and rescripting may be one of the few ways in which an adult can modify old scripts, and store new information in the subconscious. Because informa tion learned while in one state of consciousness may be more difficult to access Nancy E. To gain access to most of these statebound memories, one may have to return to the state in which they were created, that is, a theta state, that state of consciousness just above sleep character ized by a dynamic balance between the alpha and theta frequency bands. As subconscious (emotional) memories become more available to conscious (episodic) process in this deeply altered state, traumatic memories are often released and appear as fiash backs from the past. As these fiashbacks are relived in the context of current adult resources and perceptions, the subconscious memories may become more readily available for healing and alteration. Causative properties of consciousness and arousal states the reader may recall at this point that brain wave frequencies are correlated with various states of consciousness or arousal. To recapitulate briefiy, a predominance of beta waves (approximately 13Hz and higher) signals a state encompassing the thinking process with its accompanying ego reactions. In everyday existence, the ideal state of the ego may well be a state of poise between the inner world of self and the outer world of objects. With some addicts, and patients previously exposed to major trauma, alpha amplitudes can be low, creat ing an infiexibility that keeps one from shifting readily between inward and outward states (M. Patients exhibiting low alpha amplitudes may tend to avoid those internal states where one does the work to find awareness of self. As one increases alpha amplitudes via neurotherapy, such patients can gain the ability to shift with greater ease and appropriateness. Any overly intense con cern with the outer world is tempered, and the individual may gain detachment with a sense of humor and loss of egocenteredness. As one turns inward and attains deeper states, sensorimotor awareness tends to decrease, and consciousness centers on ques tions concerning the meaning of life. They seem to develop a powerful coping skill, and may have access to such inner calm no matter what is occurring in their environment (Wuttke, 1992). In such states many aspects of the self involving wisdom and insight may be encountered and awareness of earlier traumas occurs, making them more accessible for healing. The use of the term encoded patterns indicates that individuals learn certain sur vival response patterns while they are very young and the brain is still forming. These patterns are refiected in the subtle structure of the brain and are correlated with behavior. They may be considered as electrochemical circuits that respond in specified ways. The response patterns encoded in the brain of the young child lead to unconscious responses later in life, some of which may be maladaptive. As an older child or as an adult, a cognitive awareness that a certain behavior causes problems will not change the behavior until the person develops enough emotional pliability to handle that insight. The excitatory neurotransmitter glutamate has a protective effect against alcohol, and is expended in the process of reducing the effects of inebriation. Longterm potentiation refers to patterns of synaptic activity in the central nervous system that produce a long lasting increase in synaptic plasticity (laMantia and Katz, 2001). Expressed in another way, a process known as phase transition occurs in which a new neural pattern begins to take the place of the old encoded patterns (Cowan, 2008). Survival terror shuts down aspects of auto poiesis, the process of becoming, with both behavioral and, in chronic cases espe cially, measurable physiological consequences (Bower, 1996). The brain at rest tends to produce random frequency patterns, opening the door to a potential phase transition into a new pattern (Cowan, 2008), in this case one suggested by the scenario of desired outcome recited to the person during the induction phase of each session. Support in the form of adjunctive treatments and individual or group psychotherapy amplifies the new state while participation in related com munity or religious activities can provide external verification of the new state. With addiction the process appears similar to that described in the previous sec tion. The brain in its way is convinced that it cannot survive without the exogenous substance of choice or a reasonable substitute. It will cause the organism to manipu late, rationalize, avoid, lie, cheat, steal and worse to maintain the existing chemical homeostasis. Certain aspects of addictive behavior, then, may be described as affects of survival terror.
The hormones of the anterior pituitary are regulated by neuropeptides that are called either a fireleasinga or a fiinhibitinga factors or hormones gastritis diet 2 go buy clarithromycin cheap. These are produced in cell bodies in the hypothalamus gastritis zucchini cheap clarithromycin online amex, and they reach the cells of the pituitary by the hypophysial portal system ure 23 gastritis nausea cure cheap clarithromycin 250 mg line. The interaction of the releasing hormones with their receptors results in the activation of genes that promote the synthesis of protein precursors gastritis rash generic 500 mg clarithromycin with visa. These are then processed posttranslationally to the hormones and are released into the circulation gastritis diet 2 days order clarithromycin 500mg free shipping. The hypothalamicreleasing hormones are primarily used for diagnostic purposes (that is gastritis diet ����� clarithromycin 500 mg with visa, to determine pituitary insufficiency). Stress stimulates its secretion, whereas cortisol acting via negative feedback suppresses its release. This pathway ends with the synthesis and release of the adrenocorticosteroids and the adrenal androgens (see ure 23. Somatotropin influences a wide variety of biochemical processes; for example, through stimulation of protein synthetic processes, cell proliferation and bone growth are promoted. Somatotropin and somatrem should not be used in individuals with closed epiphyses or an enlarging intracranial mass. Originally isolated from the hypothalamus, somatostatin is a small polypeptide that is also found in neurons throughout the body as well as in the intestine and pancreas. Its halflife is longer than that of the natural compound, and a depot form is also available. Gallbladder emptying is delayed, and asymptomatic cholesterol gallstones can occur with longterm treatment. These are effective in suppressing production of the gonadal hormones and, thus, are effective in the treatment of prostatic cancer, P. Adverse effects of gonadorelin include hypersensitivity, dermatitis, and headache. In women, the analogs may cause hot flushes and sweating as well as diminished libido, depression, and ovarian cysts. In men, they initially cause a rise in testosterone that can result in bone pain; hot flushes, edema, gynecomastia, and diminished libido also occur. Gonadotropins: Hum an m enopausal gonadotropin, folliclestim ulating hormone, and human chorionic gonadotropin the gonadotropins are glycoproteins that are produced in the anterior pituitary. The hormone enters a cell, where it activates a tyrosine kinase to promote tyrosine phosphorylation and gene activation. On the other hand, hyperprolactinemia, which is associated with galactorrhea and hypogonadism, is usually treated with D2receptor agonists, such as bromocriptine and cabergoline. Both of these agents also find use in the treatment of microadenomas and macroprolactinomas. They not only act at the D2 receptor to inhibit prolactin secretion but also cause increased hypothalamic dopamine by decreasing its turnover. Among their adverse effects are nausea, headache, and sometimes, psychiatric problems. Hormones of the Posterior Pituitary In contrast to the hormones of the anterior lobe of the pituitary, those of the posterior lobe, vasopressin and oxytocin, are not regulated by releasing hormones. Instead, they are synthesized in the hypothalamus, transported to the posterior pituitary, and released in response to specific physiologic signals, such as high plasma osmolarity or parturition. Its only use is in obstetrics, where it is employed to stimulate uterine contraction to induce or reinforce labor or to promote ejection of breast milk. Oxytocin causes milk ejection by contracting the myoepithelial cells around the mammary alveoli. Although toxicities are uncommon when the drug is used properly, hypertensive crises, uterine rupture, water retention, and fetal death have been reported. Its antidiuretic and pressor activities are very much lower than those of vasopressin. The chemically synthesized nonapeptide has replaced that extracted from animal posterior pituitaries. In the kidney, it binds to the V2 receptor to increase water permeability and resorption in the collecting tubules. It also finds use in controlling bleeding due to esophageal varices or colonic diverticula. Other effects of vasopressin are mediated by the V1 receptor, which is found in liver, vascular smooth muscle (where it causes constriction), and other tissues. As might be expected, the major toxicities are water intoxication and hyponatremia. Caution must be used when treating patients with coronary artery disease, epilepsy, and asthma. This analog is now preferred for diabetes insipidus and nocturnal enuresis and is longeracting than vasopressin. Thyroid Hormones the thyroid gland facilitates normal growth and maturation by maintaining a level of metabolism in the tissues that is optimal for their normal function. The two major thyroid hormones are triiodothyronine (T3; the most active form) and thyroxine (T4). Although the thyroid gland is not essential for life, inadequate secretion of thyroid hormone (hypothyroidism) results in bradycardia, poor resistance to cold, and mental and physical slowing (in children, this can cause mental retardation and dwarfism). If, however, an excess of thyroid hormones is secreted (hyperthyroidism), then tachycardia and cardiac arrhythmias, body wasting, nervousness, tremor, and excess P. Thyroid hormone synthesis and secretion the thyroid gland is made up of multiple follicles that consist of a single layer of epithelial cells surrounding a lumen filled with colloid (thyroglobulin), which is the storage form of thyroid hormone. A summary of the steps in thyroid hormone synthesis and secretion is shown in ure 23. Oxidation to iodine (I2) by a peroxidase is followed by iodination of tyrosines on thyroglobulin. Mechanism of action Both T4 and T3 must dissociate from thyroxinebinding plasma proteins prior to entry into cells, either by diffusion or by active transport. In the cell, T4 is enzymatically deiodinated to T3, which enters the nucleus and attaches to specific receptors. Food, calcium preparations, and aluminumcontaining antacids can decrease the absorption of T4 but not of T3. T4 is converted to T3 by one of two distinct deiodinases, depending on the tissue. Drugs that induce the P450 enzymes, such as phenytoin, rifampin, and phenobarbital, accelerate metabolism of the thyroid hormones ure 23. Toxicity is directly related to T4 levels and manifests itself as nervousness, heart palpitations and tachycardia, intolerance to heat, and unexplained weight loss. The goal of therapy is to decrease synthesis and/or release of additional hormone. This can be accomplished by removing part or all of the thyroid gland, by inhibiting synthesis of the hormones, or by blocking release of the hormones from the follicle. Removal of part or all of the thyroid: this can be accomplished either surgically or by destruction of the gland 131 by beta particles emitted by radioactive iodine (I), which is selectively taken up by the thyroid follicular cells. Younger patients are treated with the isotope without prior pretreatment with methimazole (see below), whereas the opposite is the case in elderly patients. Most patients become hypothyroid as a result of this drug and require treatment with levothyroxine. The effects of these drugs are slow in onset; thus, they are not effective in the treatment of thyroid storm (see below). Thyroid storm: IBlockers that lack sympathomimetic activity, such as propranolol, are effective in blunting the widespread sympathetic stimulation that occurs in hyperthyroidism. An alternative in patients suffering from severe heart failure or asthma is the calcium channel blocker, diltiazem. Blockade of hormone release: A pharmacologic dose of iodide inhibits the iodination of tyrosines (the socalled a fiacute WolffChaikoff effecta ), but this effect lasts only a few days. What is more important, iodide inhibits the release of thyroid hormones from thyroglobulin by mechanisms not yet understood. However, it is employed to treat potentially fatal thyrotoxic crisis (thyroid storm) or prior to surgery, because it decreases the vascularity of the thyroid gland. Iodide is not useful for longterm therapy, because the thyroid ceases to respond to the drug after a few weeks. Adverse effects are relatively minor and include sore mouth and throat, swelling of the tongue or larynx, rashes, ulcerations of mucous membranes, and a metallic taste in the mouth. It blocks iodination and coupling of tyrosines in thyroglobulin to form thyroid hormones. Octreotide: treatment of diarrhea associated with vasoactive intestinal peptide tumors C. Overview the pancreas is both an endocrine gland that produces the peptide hormones insulin, glucagon, and somatostatin and an exocrine gland that produces digestive enzymes. These hormones play an important role in regulating the metabolic activities of the body, particularly the homeostasis of blood glucose. More commonly, a relative or absolute lack of insulin, such as in diabetes mellitus, can cause serious hyperglycemia, which, if left untreated, can result in retinopathy, nephropathy, neuropathy, and cardiovascular complications. Diabetes Mellitus the incidence of diabetes is growing rapidly both in the United States and worldwide. For example, it is estimated that more than 180 million people worldwide are afflicted with diabetes, and the prevalence is expected to more than double by the year 2030. In the United States, approximately 21 million people are estimated to suffer from diabetes, and it is a major cause of morbidity and mortality. Rather, it is a heterogeneous group of syndromes characterized by an elevation of blood glucose caused by a relative or absolute deficiency of insulin. Gestational diabetes is defined as carbohydrate intolerance with onset or first recognition during pregnancy. It is important to maintain adequate glycemic control during pregnancy, because uncontrolled gestational diabetes P. Glyburide may be a reasonably safe alternative to insulin therapy for gestational diabetes. However, larger randomized studies are needed to fully assess neonatal outcomes and optimal dosing regimens. Type 1 diabetes Type 1 diabetes most commonly afflicts individuals in puberty or early adulthood, but some latent forms can occur later in life. The disease is characterized by an absolute deficiency of insulin caused by massive Icell necrosis. Loss of Icell function is usually ascribed to autoimmune mediated processes directed against the Ifi cell, and it may be triggered by an invasion of viruses or the action of chemical toxins. As a result of the destruction of these cells, the pancreas fails to respond to glucose, and the Type 1 diabetic shows classic symptoms of insulin deficiency (polydipsia, polyphagia, polyuria, and weight loss). Type 1 diabetics require exogenous insulin to avoid the catabolic state that results from and is characterized by hyperglycemia and lifethreatening ketoacidosis. Cause of Type 1 diabetes: In the postabsorptive period of a normal individual, low, basal levels of circulating insulin are maintained through constant Icell secretion. A burst of insulin secretion occurs within 2 minutes after ingesting a meal, in response to transient increases in the levels of circulating glucose and amino acids. This lasts for up to 15 minutes, and, is followed by the postprandial secretion of insulin. However, having virtually no functional Ifi cells, the Type 1 diabetic can neither maintain a basal secretion level of insulin nor respond to variations in circulating fuels ure 24. The development and progression of neuropathy, nephropathy, and retinopathy are directly related to the extent of glycemic control (measured as blood levels of glucose and/or hemoglobin A [HbA ]). Treatment: A Type 1 diabetic must rely on exogenous (injected) insulin to control hyperglycemia, avoid ketoacidosis, and maintain acceptable levels of glycosylated hemoglobin (HbA1c). The use of home blood glucose monitors facilitates frequent selfmonitoring and treatment with insulin injections. This method of administration may be more convenient for some patients, eliminating the multiple daily injections of insulin. Other methods of insulin delivery, such as transdermal, buccal, and intranasal, are currently under investigation. Amylin is a hormone that is cosecreted with insulin from pancreatic Ifi cells following food intake. The disease is influenced by genetic factors, aging, obesity, and peripheral insulin resistance rather than by autoimmune processes or viruses. The metabolic alterations observed are milder than those described for Type 1 (for example, Type 2 patients typically are not ketotic), but the longterm clinical consequences can be just as devastating (for example, vascular complications and subsequent infection can lead to amputation of the lower limbs). Cause: In Type 2 diabetes, the pancreas retains some Icell function, but variable insulin secretion is insufficient to maintain glucose homeostasis (see ure 24. This resistance to insulin is considered to be a major cause of this type of diabetes. Treatment: the goal in treating Type 2 diabetes is to maintain blood glucose concentrations within normal limits and to prevent the development of longterm complications of the disease. Weight reduction, exercise, and dietary modification decrease insulin resistance and correct the hyperglycemia of Type 2 diabetes in some patients. However, most patients are dependent on pharmacologic intervention with oral hypoglycemic agents. As the disease progresses, Icell function declines, and insulin therapy is often required to achieve satisfactory serum glucose levels ure 24. It is synthesized as a precursor (proinsulin) that undergoes proteolytic cleavage to form insulin and C peptide, both of which are secreted by the Ifi cells of the pancreas. Because radioimmunoassays do not distinguish between proinsulin and insulin, Type 2 patients may have lower levels of the active hormone than the assay indicates. Thus, measurement of circulating C peptide provides a better index of insulin levels.
Purchase clarithromycin american express. Is popcorn safe to eat with a ulcer ? | Health FAQs.
References
- Connelan JM, Thurlow PJ, Barlow B, et al. Investigation of alternative mechanisms of collagen-induced platelet activation using monoclonal antibodies to glycoprotein 11b-111a and fibrinogen. Thromb. Haemost 1986;55:153-57.
- Laing NG, Laing BA, Meredith C, et al. Autosomal dominant distal myopathy: Linkage to chromosome 14.
- Nelson LM, Maguire V, Longstreth WT Jr, Matkin C. Population- based case control study of amyotrophic lateral sclerosis in western Washington State I. Cigarette smoking and alcohol consumption. Am J Epidemol. 2000;151:156-163.
- Shoham S, Pic-Aluas L, Taylor J, et al. Pulmonary Ochroconis gallopavum infections. Transplant Infect Dis. 2008;10:442-448.
- Vetro C, Romano A, Chiarenza A, et al. Endoscopic ultrasonography in gastric lymphomas: appraisal on reliability in longterm follow-up. Hematol Oncol. 2012;30:180-185.